1/P
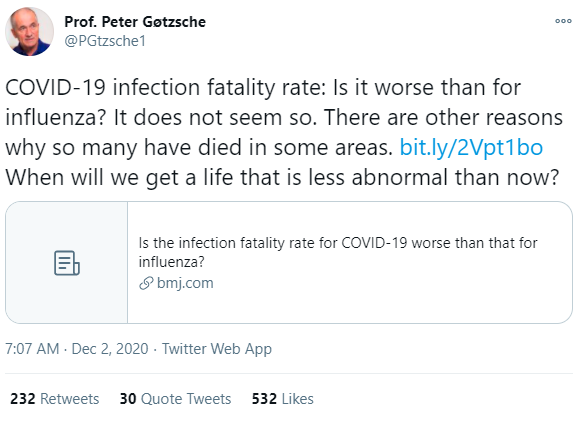
Peter C Gøtzsche (@PGtzsche1) wrote the article below
He argues that COVID-19 isn't very lethal, + then draws some political conclusions.
The article is poor.
"Is the infection fatality rate for COVID-19 worse than that for influenza?"
bmj.com/content/371/bm…
Peter C Gøtzsche (@PGtzsche1) wrote the article below
He argues that COVID-19 isn't very lethal, + then draws some political conclusions.
The article is poor.
"Is the infection fatality rate for COVID-19 worse than that for influenza?"
bmj.com/content/371/bm…
2/P
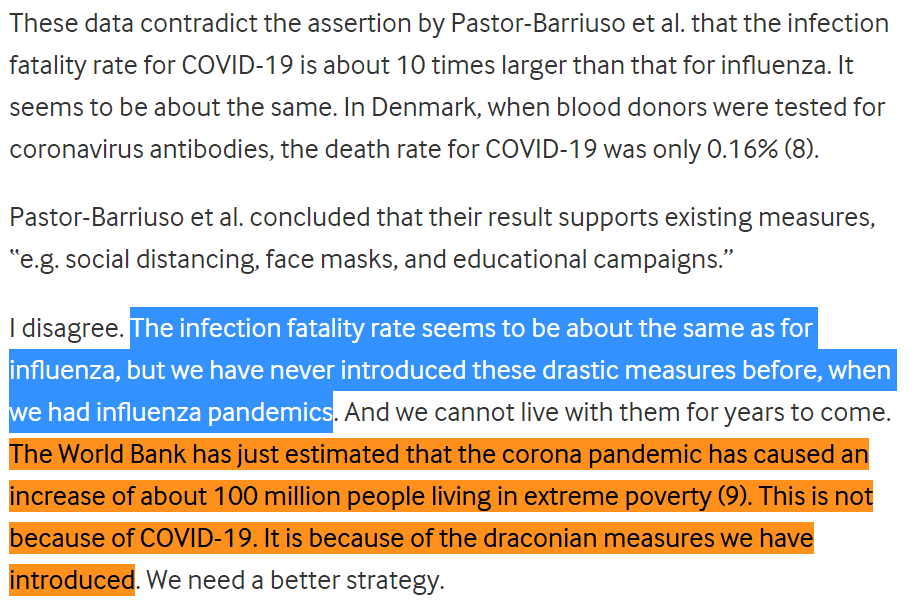
Gøtzsche's basic idea is:
The proportion of SARS-CoV-2-infected people who die of the disease COVID-19 is comparable to that of flu; i.e. the infection fatality rate (IFR) for COVID-19 is not an order of magnitude larger than that of the flu.
So:
bmj.com/content/371/bm…
Gøtzsche's basic idea is:
The proportion of SARS-CoV-2-infected people who die of the disease COVID-19 is comparable to that of flu; i.e. the infection fatality rate (IFR) for COVID-19 is not an order of magnitude larger than that of the flu.
So:
bmj.com/content/371/bm…
3/P
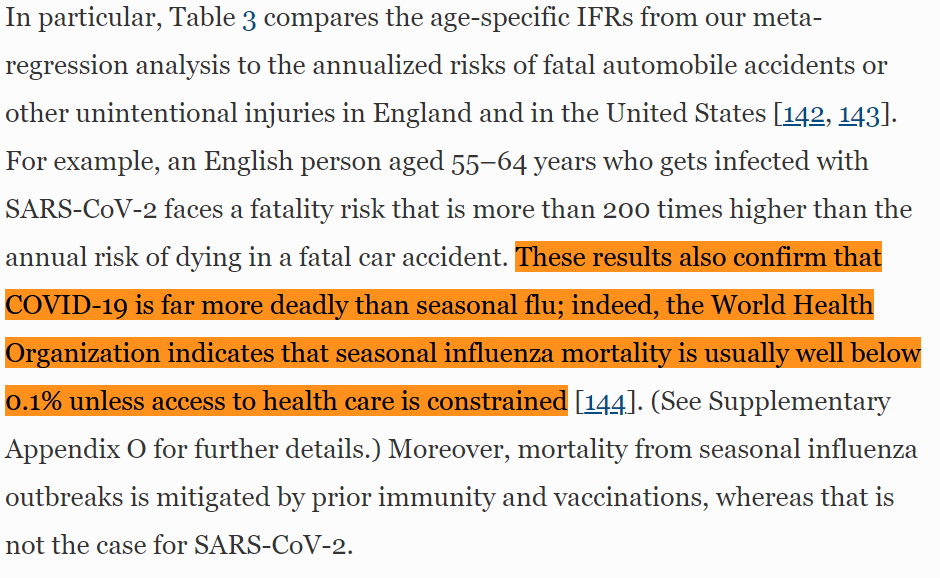
Gøtzsche is wrong. Study after study shows that the fatality rate for SARS-CoV-2 is about an order of magnitude larger than that of influenza; COVID-19 is way more dangerous than the flu.
So where does Gøtzsche go wrong?
link.springer.com/article/10.100…
Gøtzsche is wrong. Study after study shows that the fatality rate for SARS-CoV-2 is about an order of magnitude larger than that of influenza; COVID-19 is way more dangerous than the flu.
So where does Gøtzsche go wrong?
https://twitter.com/AtomsksSanakan/status/1299429571058696194
link.springer.com/article/10.100…
4/P
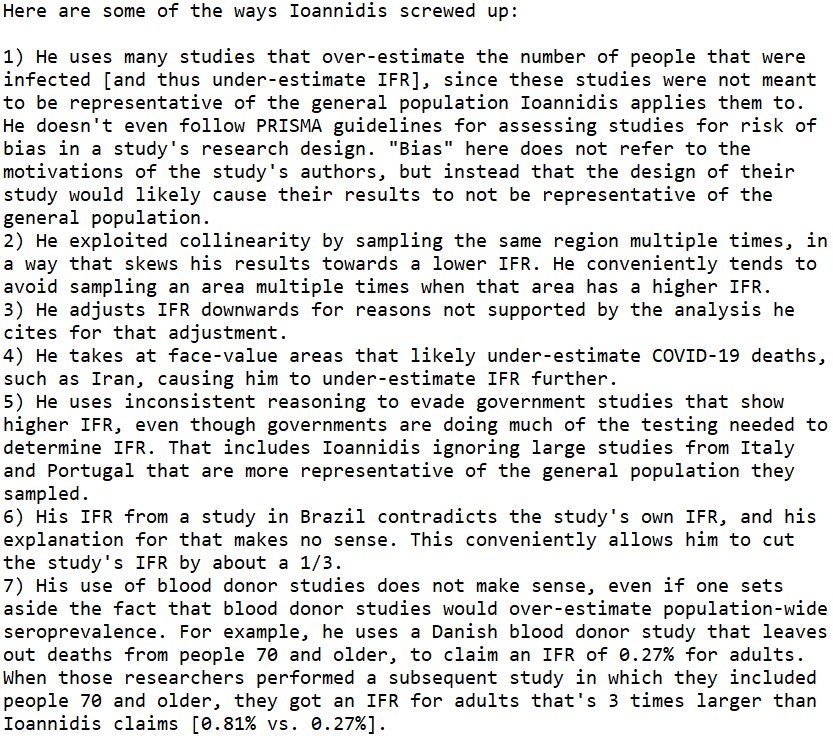
Gøtzsche cites a dubious meta-analysis from John Ioannidis, who under-estimates SARS-CoV-2's IFR.
rapidreviewscovid19.mitpress.mit.edu/pub/p6tto8hl/r…
hildabastian.net/index.php/91
Gøtzsche cites a dubious meta-analysis from John Ioannidis, who under-estimates SARS-CoV-2's IFR.
rapidreviewscovid19.mitpress.mit.edu/pub/p6tto8hl/r…
hildabastian.net/index.php/91
https://twitter.com/AVG_Joseph96/status/1283234509639618560
https://twitter.com/AtomsksSanakan/status/1321081788517752832
https://twitter.com/AtomsksSanakan/status/1272361132527955968
https://twitter.com/GidMK/status/1316511734115385344
5/P
Gøtzsche calls this, "a 2020 review by John Ioannidis, which is in press in the Bulletin of the World Health Organization."
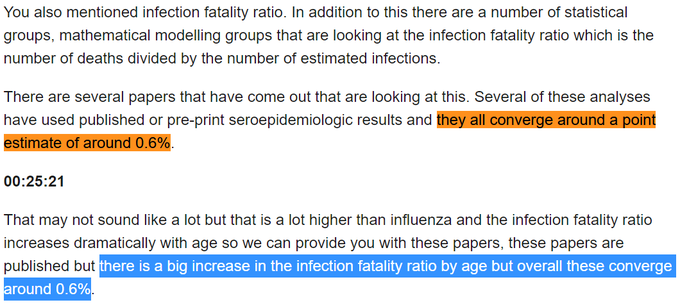
Interestingly, the World Health Organization does not agree with Gøtzsche.
October 12:
who.int/publications/m…
Gøtzsche calls this, "a 2020 review by John Ioannidis, which is in press in the Bulletin of the World Health Organization."
Interestingly, the World Health Organization does not agree with Gøtzsche.
https://twitter.com/AtomsksSanakan/status/1290693682602156046
October 12:
who.int/publications/m…
6/P
Gøtzsche then cites his book to say the CDC may be unreliable on influenza's IFR.
But the CDC doesn't give an influenza IFR. They give a case fatality rate (CFR), where reported cases are limited to symptomatic illnesses
cdc.gov/flu/about/burd…
See:
Gøtzsche then cites his book to say the CDC may be unreliable on influenza's IFR.
But the CDC doesn't give an influenza IFR. They give a case fatality rate (CFR), where reported cases are limited to symptomatic illnesses
cdc.gov/flu/about/burd…
See:
7/P
Influenza IFR can be calculated from the CFR, yielding an IFR of <0.1%. That extends beyond the CDC.
who.int/emergencies/di…
ncbi.nlm.nih.gov/pmc/articles/P…
static-content.springer.com/esm/art%3A10.1…
Influenza IFR can be calculated from the CFR, yielding an IFR of <0.1%. That extends beyond the CDC.
who.int/emergencies/di…
ncbi.nlm.nih.gov/pmc/articles/P…
https://twitter.com/AtomsksSanakan/status/1312367322837987328
https://twitter.com/mlipsitch/status/1251521082542211074
https://twitter.com/AdamJKucharski/status/1243466404415909889
https://twitter.com/AtomsksSanakan/status/1322365905595179015
static-content.springer.com/esm/art%3A10.1…
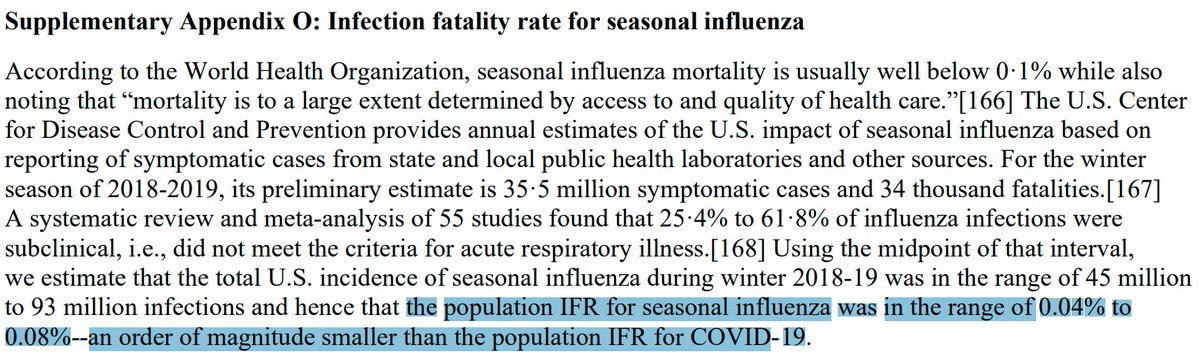
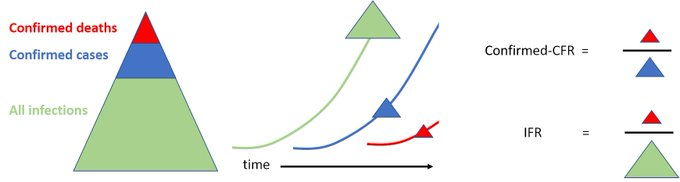
8/P
Gøtzsche goes on to compare *CFRs* from other pathogens to the *IFR* of SARS-CoV-2. That's misleading since IFR is less than, or equal to, CFR. In fact, IFR is almost always less than CFR, since CFR misses some infections.
institutefordiseasemodeling.github.io/nCoV-public/an…
Gøtzsche goes on to compare *CFRs* from other pathogens to the *IFR* of SARS-CoV-2. That's misleading since IFR is less than, or equal to, CFR. In fact, IFR is almost always less than CFR, since CFR misses some infections.
institutefordiseasemodeling.github.io/nCoV-public/an…
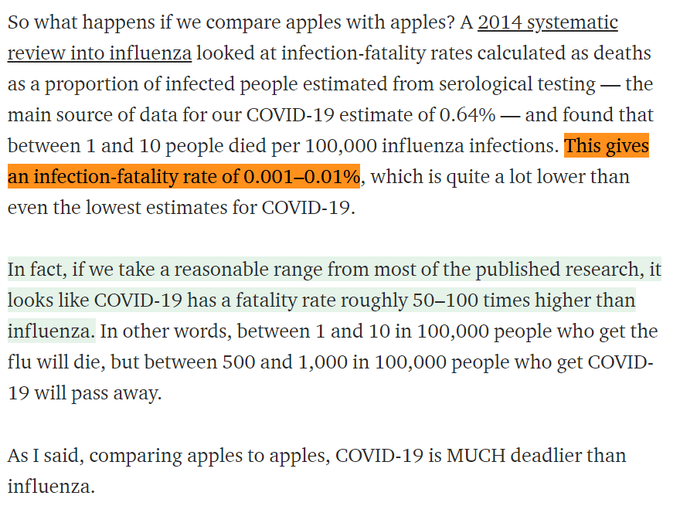
9/P
A good illustration of this is Gøtzsche comparing SARS-CoV-2's *IFR* to a 1% *CFR* for the 2009 pandemic flu.
But the 2009 pandemic's *IFR* was around two or three orders of magnitude less
ncbi.nlm.nih.gov/pmc/articles/P…
From @GidMK:
medium.com/@gidmk/covid-1…
A good illustration of this is Gøtzsche comparing SARS-CoV-2's *IFR* to a 1% *CFR* for the 2009 pandemic flu.
But the 2009 pandemic's *IFR* was around two or three orders of magnitude less
ncbi.nlm.nih.gov/pmc/articles/P…
https://twitter.com/AtomsksSanakan/status/1307562794770927617
From @GidMK:
medium.com/@gidmk/covid-1…
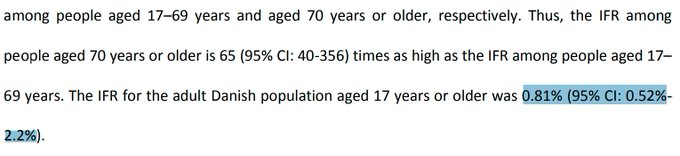
10/P
Gøtzsche cites a blood donor research to claim a SARS-CoV-2 IFR of 0.16%. That's:
- cherry-picking
- using a type of study that under-estimates IFR for multiple reasons
- citing a source that doesn't give an IFR
- the research implies a larger IFR
Gøtzsche cites a blood donor research to claim a SARS-CoV-2 IFR of 0.16%. That's:
- cherry-picking
- using a type of study that under-estimates IFR for multiple reasons
- citing a source that doesn't give an IFR
- the research implies a larger IFR
https://twitter.com/AtomsksSanakan/status/1321081788517752832
11/P
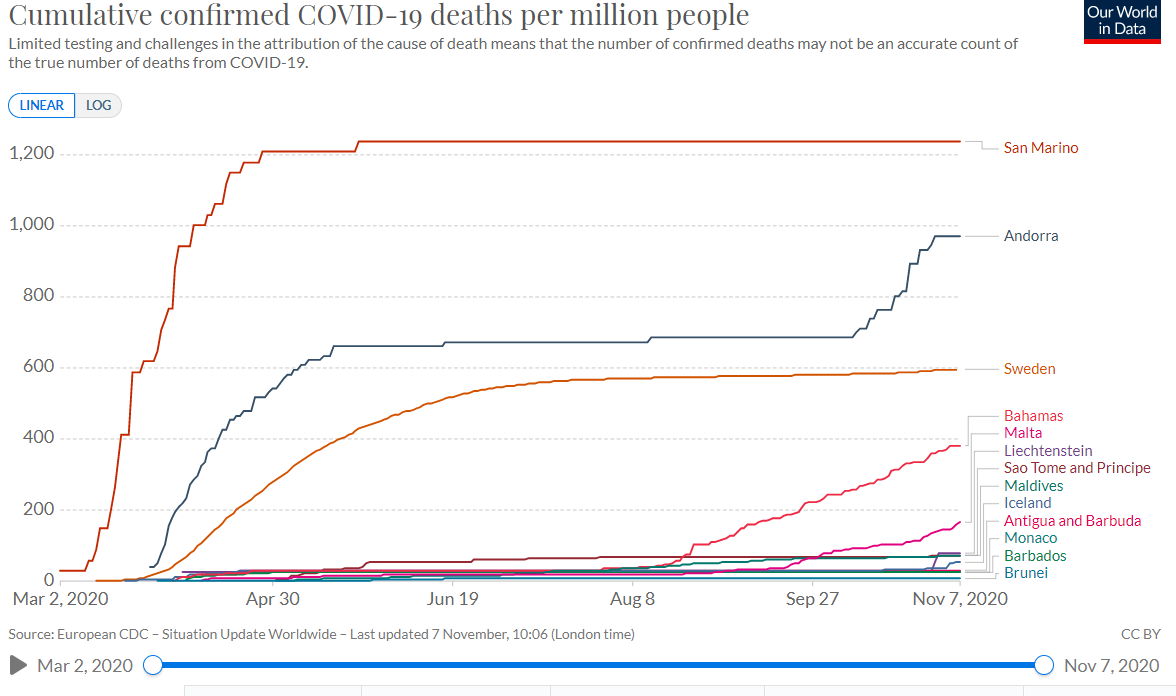
Evidence also does not support Gøtzsche's claim that "draconian measures" (🙄; see part 2/P) in response to COVID-19 caused poverty, not COVID-19.
For example, Sweden's less stringent response wasn't better in terms of GDP:
Evidence also does not support Gøtzsche's claim that "draconian measures" (🙄; see part 2/P) in response to COVID-19 caused poverty, not COVID-19.
For example, Sweden's less stringent response wasn't better in terms of GDP:
https://twitter.com/AtomsksSanakan/status/1325490855197683712
https://twitter.com/AtomsksSanakan/status/1302850348822990848

12/P
Gøtzsche's article is thus filled with false claims and distortions, leading to his politically-motivated conclusion.
But how could he do this? He should have the biological knowledge to see his claims are wrong.
en.wikipedia.org/wiki/Peter_C._…
Gøtzsche's article is thus filled with false claims and distortions, leading to his politically-motivated conclusion.
But how could he do this? He should have the biological knowledge to see his claims are wrong.
en.wikipedia.org/wiki/Peter_C._…
13/P
One plausible explanation is that Gøtzsche's ideological opposition to some policy responses to COVID-19, pushed him to contrarianism on COVID-19. His contrarian tendencies appeared before, just as with John Ioannidis:
en.wikipedia.org/wiki/Peter_C._…
One plausible explanation is that Gøtzsche's ideological opposition to some policy responses to COVID-19, pushed him to contrarianism on COVID-19. His contrarian tendencies appeared before, just as with John Ioannidis:
https://twitter.com/AtomsksSanakan/status/1272672360416579589
en.wikipedia.org/wiki/Peter_C._…
14/P
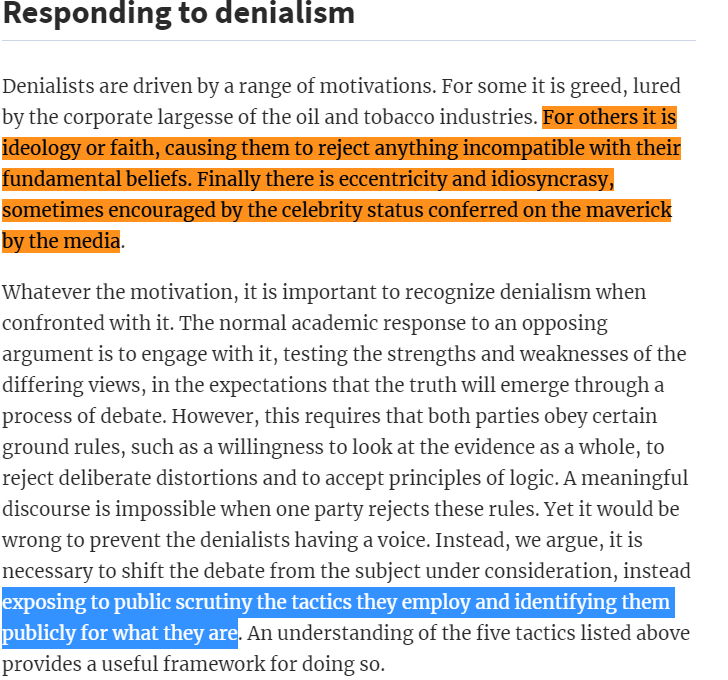
So the COVID-19 pandemic brought out ideologically-motivated contrarianism and denialism, just like the AIDS pandemic, anthropogenic climate change, vaccination, GMOs, etc. did.
How unfortunate.
academic.oup.com/eurpub/article…
So the COVID-19 pandemic brought out ideologically-motivated contrarianism and denialism, just like the AIDS pandemic, anthropogenic climate change, vaccination, GMOs, etc. did.
How unfortunate.
https://twitter.com/ClimateOfGavin/status/1259267627471507456
academic.oup.com/eurpub/article…
15/P
And below is a thread in which Gøtzsche's promotes the article I criticized:
And below is a thread in which Gøtzsche's promotes the article I criticized:
https://twitter.com/PGtzsche1/status/1334106917690544133
16/P
Others pointed out this contrarianism long before I did.
An early example from one of my role models:
Others pointed out this contrarianism long before I did.
An early example from one of my role models:
https://twitter.com/gorskon/status/1242818039374131200

• • •
Missing some Tweet in this thread? You can try to
force a refresh