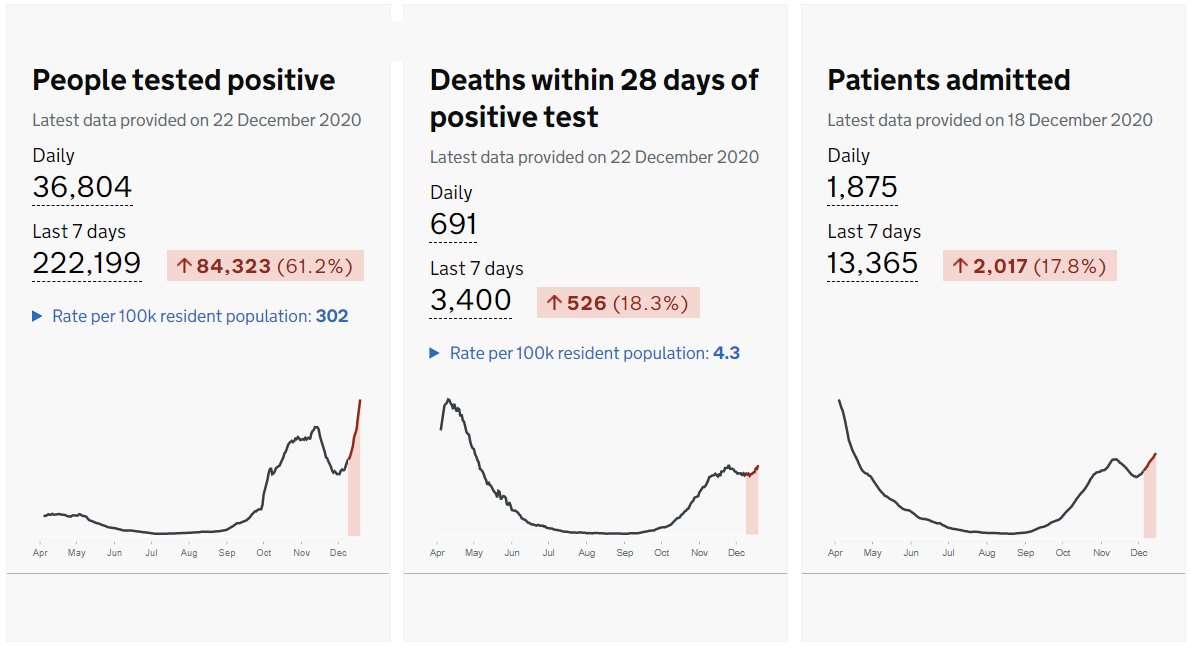
The number of new coronavirus infections may be levelling off, but patient admissions to NHS hospitals for COVID-19 will increase for another 7-10 days. The question of how we choose which patient gets an ICU bed is now a routine one in media interviews. Doctors are worried. 1/11 

The burden of decision making around ICU admission traditionally falls on senior ICU doctors. Most of us are privately very worried about what will happen if we run out of resources. The false suggestion that we rationed ICU beds in the first wave has upset a lot of people. 2/11
To be clear, I am not aware of ANY patient who was not admitted to intensive care during the pandemic when the ICU consultants responsible believed that they should be. But we would be failing in our duty if we do not plan for this situation. 3/11

We already have a framework for this scenario. @ICSupdates developed CRITCON levels from 0 (able to meet all ICU needs) up to 4 (services overwhelmed). Each level has principles for decision making which map to patient numbers and available resources. 4/11 journals.sagepub.com/doi/full/10.11…
But while the CRITCON levels are valuable in describing the scenarios and ethical principles of decision making, they do not give doctors a set of rules to follow. Our decisions remain subjective, individual and personal. We are lacking guidance from society. 5/11
Doctors are especially fearful of ‘Moral distress’ - the experience healthcare staff have when they know the right thing to do for a patient but ‘institutional’ constraints make this impossible. This from @mancunianmedic. 6/11 bmj.com/content/360/bm…
As well as moral distress, families may challenge our decisions. This alone is stressful but there is also fear of litigation, professional sanction and other impacts on our professional lives. If doctors are afraid to make decisions it will be worse for everyone. 7/11
Today’s statement from @Nuffbioethics is timely and welcome. Doctors want society's guidance so we know we are doing our best. The statement calls for action from government but we must understand that they too can experience moral injury. 8/11
nuffieldbioethics.org/news/statement…
nuffieldbioethics.org/news/statement…
Earlier in the pandemic @ICS_updates released advice to support decision-making. This is now being reviewed and updated. A key point for doctors: we should never choose between patients unless CRITCON level 4 is declared at a national level. 9/11
@ICS_updates president @stephen_t_webb commented on the @Nuffbioethics statement and reminded the public that ICU doctors make difficult decisions every day for individual patients. But we never want to choose *between* patients. Many doctors would like official guidance. 10/11
Meanwhile, I strongly recommend this website from @danjrharvey and @dalecgardiner at @NUHCriticalCare. It explains the ethical framework and gives genuine practical examples which are relevant to my experiences in hospital. 11/11
moralbalance.org/framework/
moralbalance.org/framework/
• • •
Missing some Tweet in this thread? You can try to
force a refresh