Self-reflection after reading @Retlouping blog on clinical testing to see if I understand the principles. In plain language.
https://twitter.com/Retlouping/status/1350922023300714498
Pre-test probability = Your % confidence that the patient has the diagnosis BEFORE clinical testing (still a bit unclear how this is calculated)
Post-test probability = Your confidence that the patient has the diagnosis AFTER clinical testing
So far so good I think.
Post-test probability = Your confidence that the patient has the diagnosis AFTER clinical testing
So far so good I think.
Preferably we are looking for a big shift in confidence either in a positive or negative direction.
A shift in a positive direction means u are more confident that the diagnosis IS present.
A shift in a negative direction means u are more confident that the diagnosis is NOT present.
A shift in a negative direction means u are more confident that the diagnosis is NOT present.
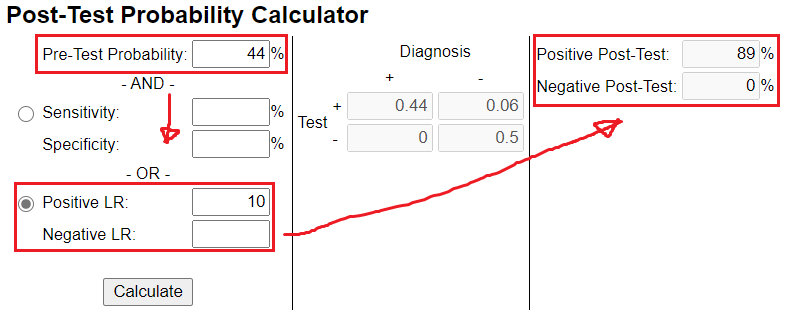
Our post-test probability has the greatest shift in probability with tests that either have a high (>10) or low (<0.1) likelihood ratio (LHR). 

It's important to choose clinical tests that improves upon your pre-test probability. If u choose a test with a LHR of 1, u end up with a zero % change in your post-test probability (see image).
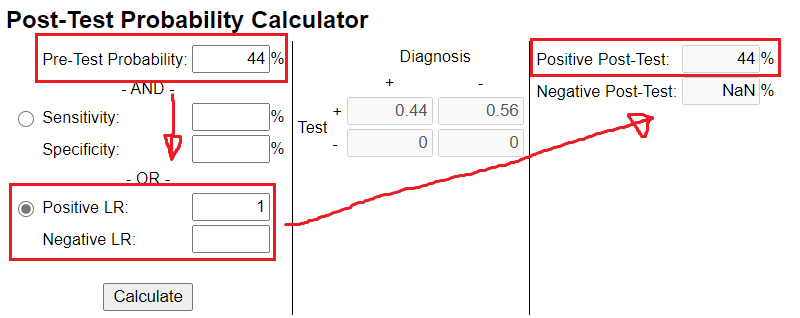
In other words, even if your next clinical test is positive it should do NOTHING to your confidence because it does not have the ability to change it.
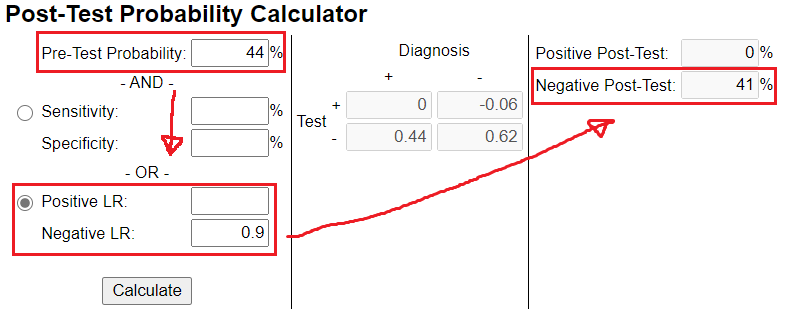
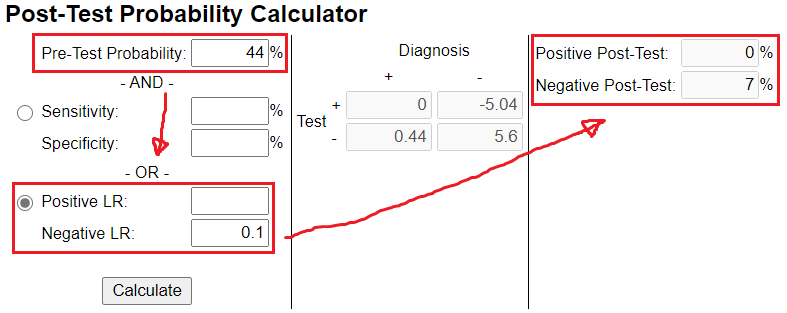
If u choose a test with a likelihood ratio below 1 your post-test probability is decreased (see image)
Watch what happens with a LHR of 5 (moderate change in probability)
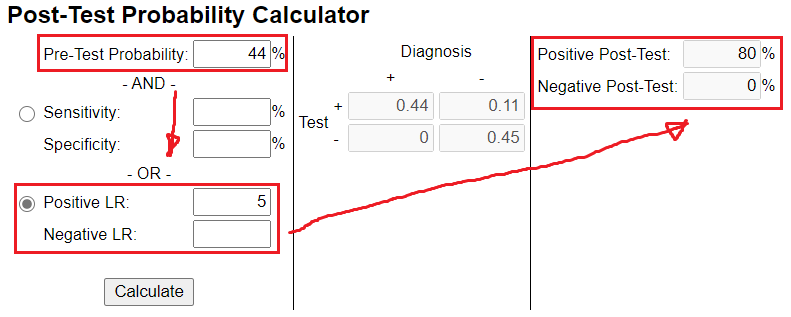
And a LHR of 10 (often large or conclusive shift in probability)
If u choose a LHR that has the ability to greatly decrease your confidence in the given diagnosis, it could look something like this. Your post-test confidence was decreased from 44 % to 7 %. In other words, it's highly likely that the diagnosis is NOT present.
I would appreciate all corrections on this thread!
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh