
Thank you to @AJPRenal, to Drs. Zachary Gray (superstar) @StanfordMedRes , Wanzhu Tu, @gchertow, and for ongoing dialogue Dr. Howard Pratt for the opportunity to articulate this concept. 1/13
Many investigators have referenced aldosterone sensitivity. Dr. Wanzhu Tu first employed the term with Dr. Howard Pratt and with the incomparable Dr. John Funder in 2014. pubmed.ncbi.nlm.nih.gov/24711519/ @HyperAHA 2/13
Training with Dr. David Pearce @UCSFNephrology , we studied aldosterone-mediated ion transport, but seeing patients with a phenotype of low-renin resistant hypertension- with a normal, but non-suppressed #aldosterone , I started thinking about this more. 3/13
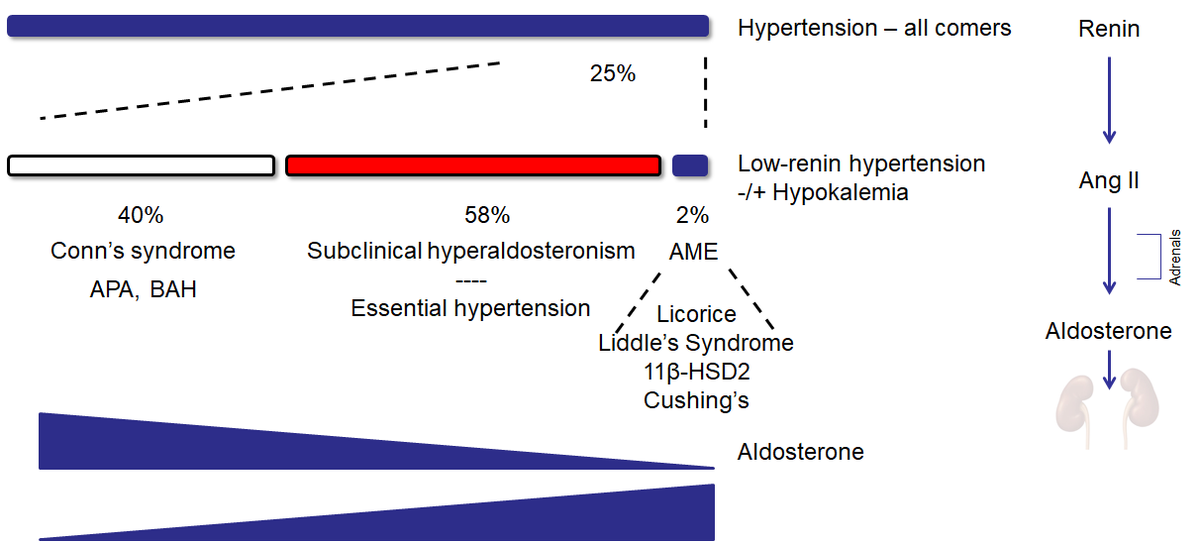
Work from @JeniferBrown @AnandVaidya17 @AnnalsofIM has taught us that there is a spectrum of non-suppressed aldosterone in low-renin hypertension; some with obvious Conn's syndrome, but many more with a lower aldo, yet still severe hypertension 4/13 
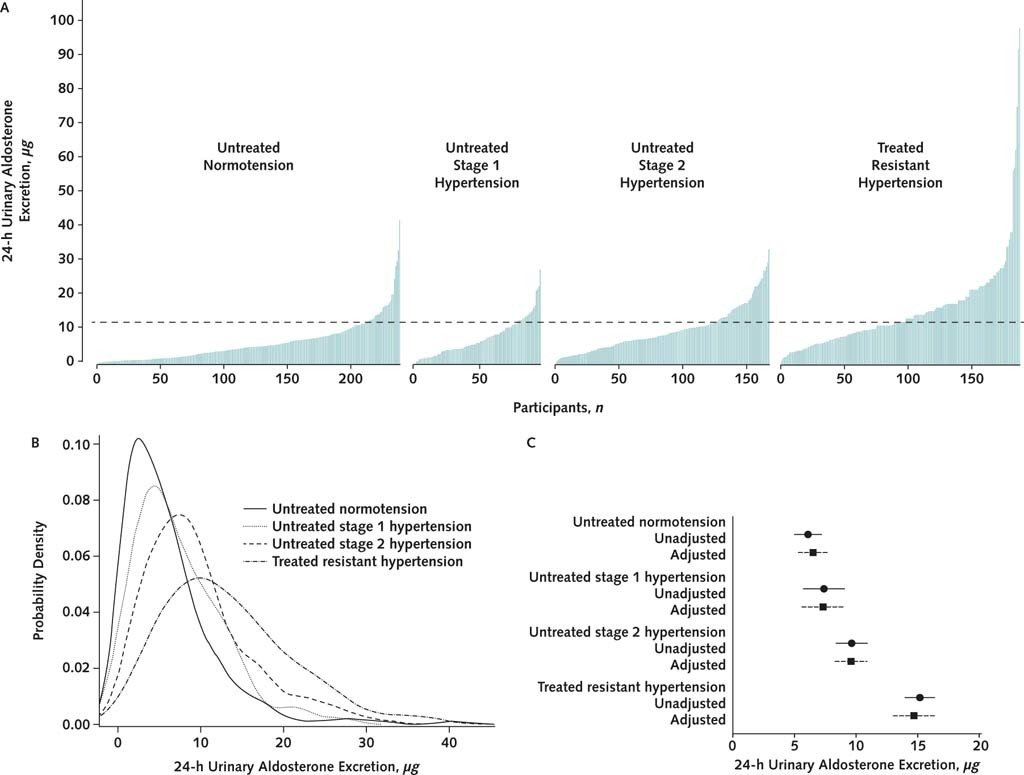
While aldo levels are high and induce HTN in Conn's syndrome, and licorice/Liddle's and other more uncommon conditions can generate HTN downstream of aldosterone, how do we address the largest group in the middle? 5/13
More than 40 years ago, Drs. Adam, Funder, and colleagues elegantly demonstrated that pts w/ severe HTN have a six-fold spectrum of response to a fixed dose of aldosterone, and that response can vary across patients, but is shared across organs within the same patient. 6/13
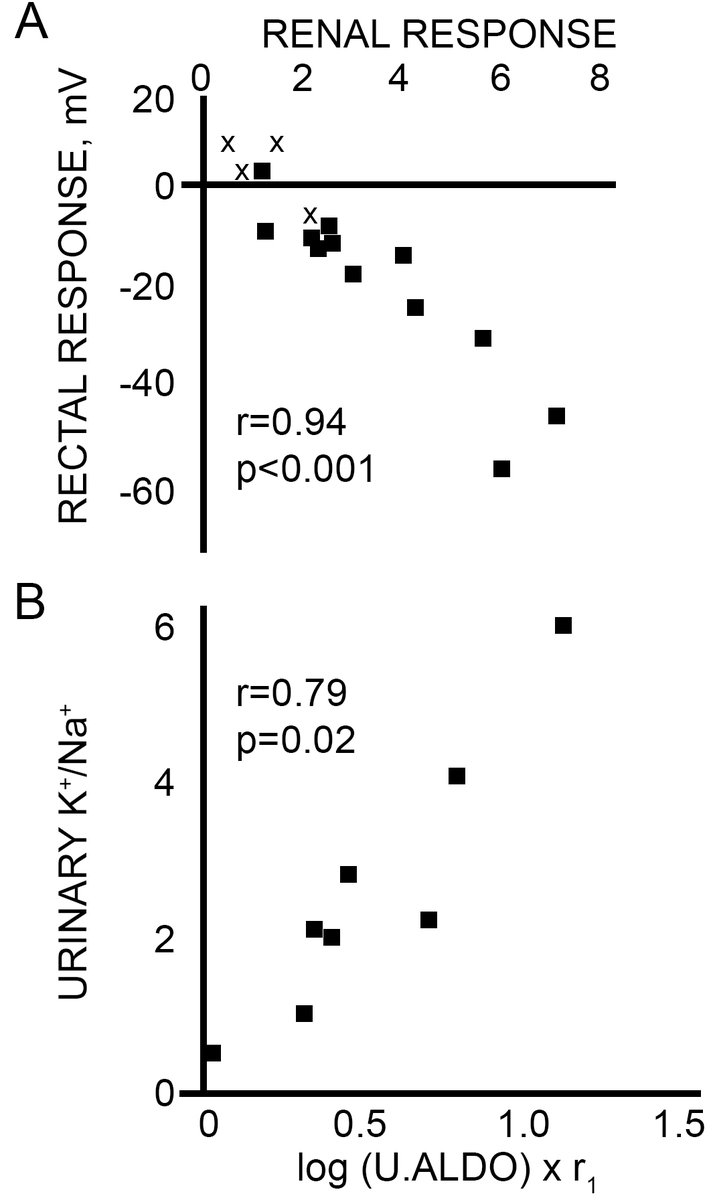
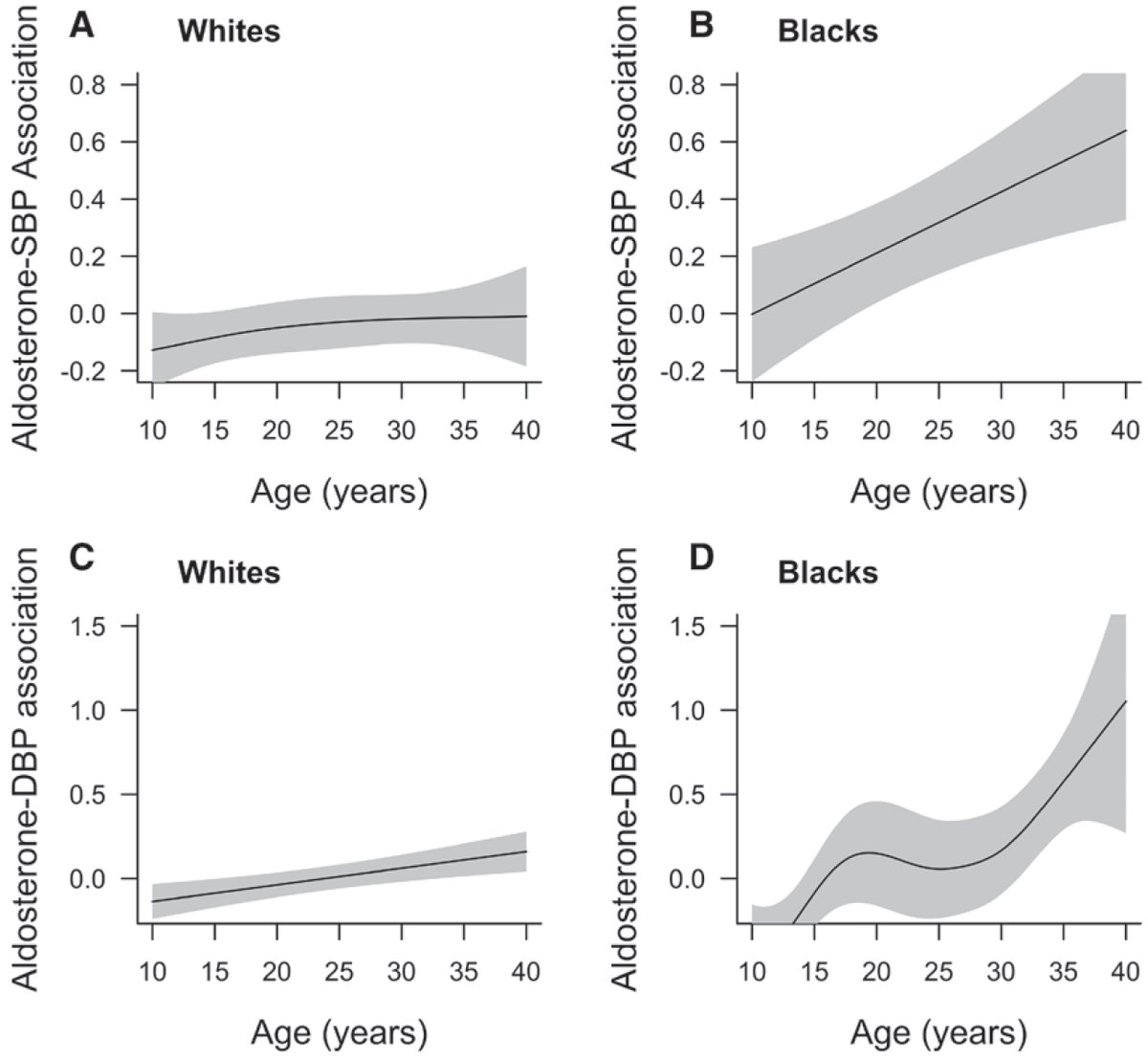
Drs. Tu and Pratt showed that the level of blood pressure (and response to aldosterone) can vary with race/ethnic background and with age. 7/13
Dr. Bryan Williams in PATHWAY-2 @TheLancet @TheLancetEndo also show that among patients with resistant hypertension and normal aldosterone, low-renin state predicted a higher response to MRAs AND to amiloride. 8/13
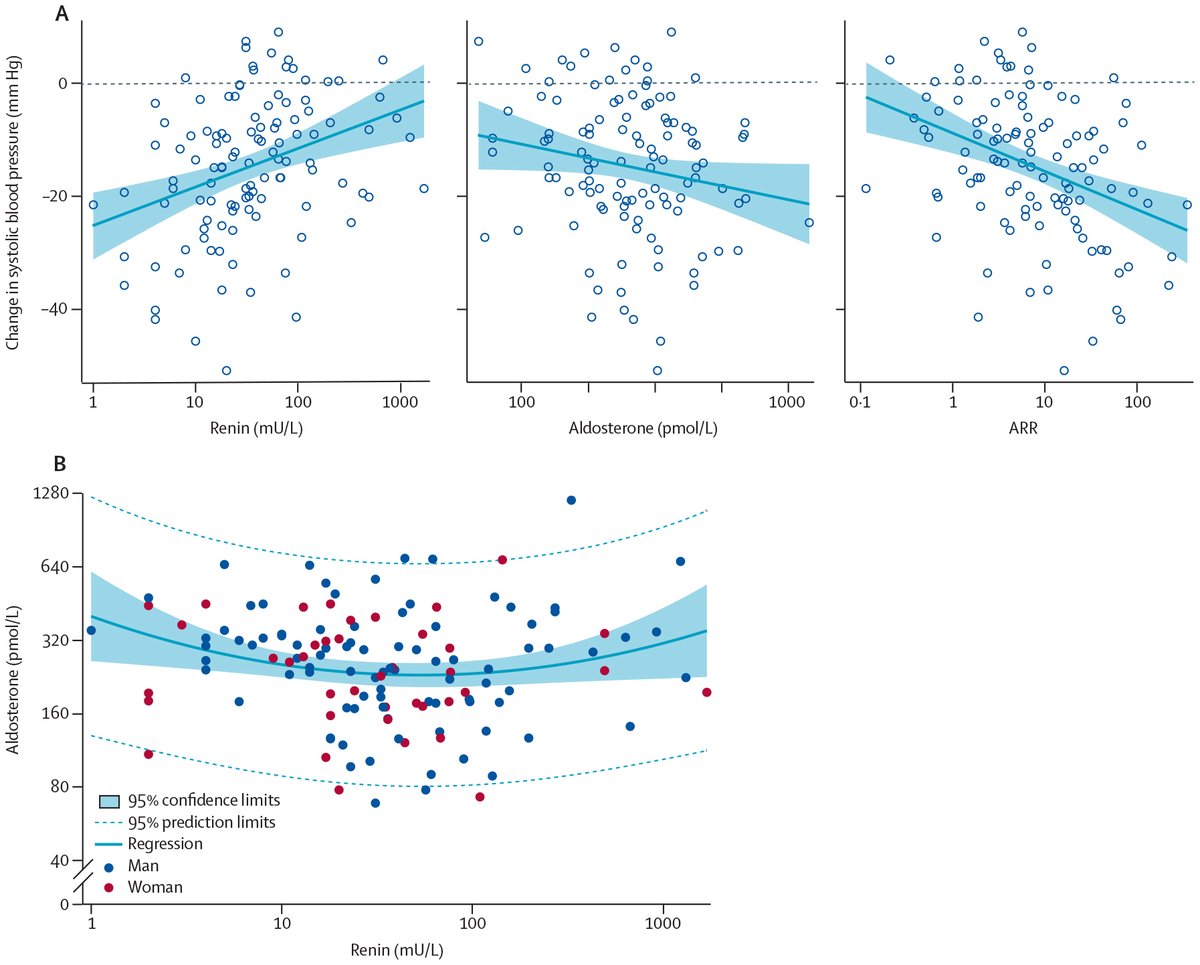
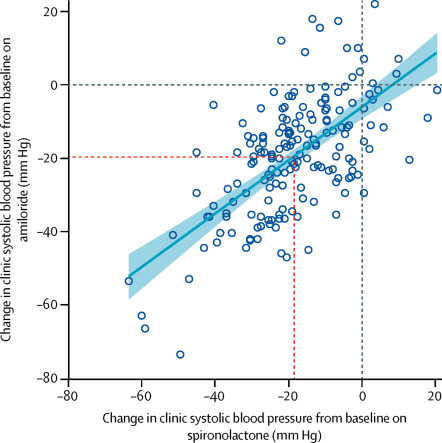
This effect may be unrecognized primary or subclinical hyperaldosteronism, the variation in aldo and the known variation in sensitivity to aldo / MRA response / ENaC inhibition, argues that there are factors downstream of aldosterone that CAN possibly modulate the response. 9/13
Not all aldosterone is treated equally. There are several possible explanations for these observations, but there is merit in questioning our threshhold for elevated aldo as advocated by @AnandVaidya17 and for considering the hypothesis that variations in... 10/13
MR signaling, such as Rac1, MR phosphorylation, MR ubiquitination, SGK1 activity, length of the CCD, etc. may cause resistant HTN with a minimum but independent, APCC / aldo production in one pt, yet another pt develops HTN only when aldosterone production is far higher. 11/13
I fully agree that we already have MRAs and amiloride, so why bother? (1) These drugs are underprescribed, (2) our 'high aldo' threshhold may need to be individualized to not miss Conn's in others; (3) understanding mechanism can always help to better address hypertension. 12/13
To translate these concepts we need to assess these pathways across race/ethnicity (e.g. urinary exosomes, @thebyrdlab; genetics) and to consider the range of aldo response in this large subcohort of 'essential' hypertension. Welcome your feedback & open to collaboration. 13/13
• • •
Missing some Tweet in this thread? You can try to
force a refresh


