
Many are interpreting data from Denmark as strong evidence of increased transmissibility of B117.
With the caveat that I believe this prevailing hypothesis to be credible, if not likely...
A thread on how Danish data can be explained w/o invoking increase in transmissibility.
With the caveat that I believe this prevailing hypothesis to be credible, if not likely...
A thread on how Danish data can be explained w/o invoking increase in transmissibility.
First, Denmark should be applauded for their rigorous genomic surveillance. Other countries should follow their example!
The data, in brief, show an increase in the percentage of sequenced cases that are B117, from 0.2% in early December to (prelim) 12% in mid-Jan.
The data, in brief, show an increase in the percentage of sequenced cases that are B117, from 0.2% in early December to (prelim) 12% in mid-Jan.
This was, however, occurring in the context of a dramatic fall in cases throughout the country, likely reflecting the effects of a country-wide lockdown. 
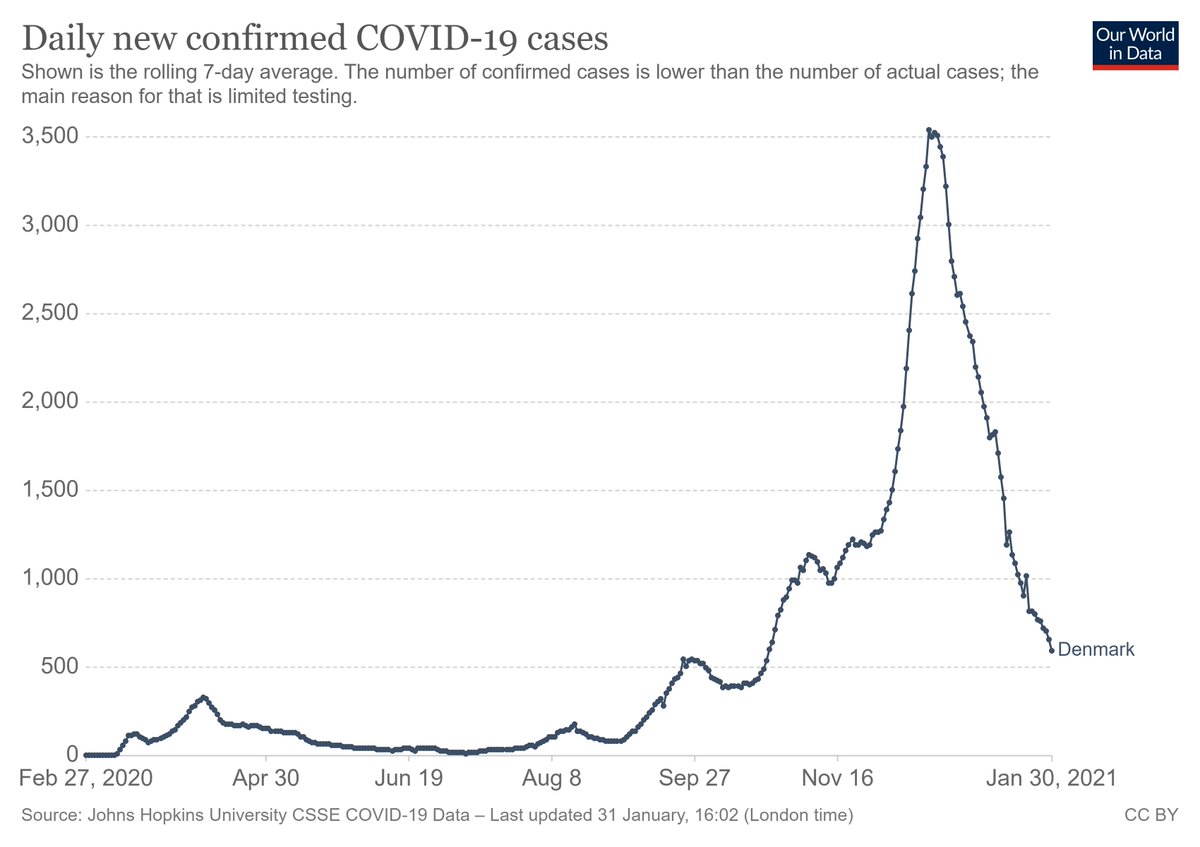
Looking at the data another way - as (# of cases in the last 2 weeks)/(# of cases the 2 weeks before this), the drop in cases in Jan 2021 was at least as steep - if not more - than with the initial lockdown in Apr/May 2020. Despite B117.

For the first 2 weeks of Jan, while cases as a whole were falling, the number of B117 cases was essentially flat (224 in the 2nd week of Jan., 231 cases in the 3rd week).
This has been interpreted by models as consistent w/ 20-50% higher transmissibility.
This has been interpreted by models as consistent w/ 20-50% higher transmissibility.
But these estimates do not account for the possibility (likelihood?) that B117 may be circulating in populations with more mixing - crowded, traveling, essential workers, etc.
Think of how B117 likely made it to Denmark...likely w people/in contexts w higher-than-average mixing.
Think of how B117 likely made it to Denmark...likely w people/in contexts w higher-than-average mixing.
A simple illustrative example - consider a population w/ 2 groups: low-mixing (0.5 secondary cases per infected person) & high-mixing (1.25 secondary cases).
Ignoring herd immunity, w/ 2 low-mixing cases per high-mixing case, we will see 0.75 secondary cases per infected person.
Ignoring herd immunity, w/ 2 low-mixing cases per high-mixing case, we will see 0.75 secondary cases per infected person.

Let's see what happens in this declining epidemic with each generation, comparing the red strain (equal transmissibility, but seeded in the high-mixing group) to the other (blue) cases.
After 1 generation, the total number of cases is falling, but the fraction red is rising.
After 1 generation, the total number of cases is falling, but the fraction red is rising.

As long as the red strain continues to circulate in the high-mixing group (not accounting for possible re-introduction - likely in Denmark as long as B117 remains the dominant strain in a nearby country), the # of red cases can remain stable, even as total cases fall.

In this simple illustration, after 3 generations, the # of red cases is still the same, even as the total # of cases has fallen by 2/3. This need not invoke any increased transmissibility of the red strain.
Very similar to current Danish data on B117.
Very similar to current Danish data on B117.

All this to say, increased transmissibility is not the only viable explanation for stable B117 cases while total cases decline. Heterogeneity in mixing patterns - w B117 circulating in higher-mixing populations - can also explain these data.
These patterns would also be consistent w/ higher contact positivity in people w B117 (as seen in the UK). If people w B117 mix more closely w their contacts, on average, then more of those contacts are likely to be infected.
Also, as I've suggested before, the most likely explanation is a combination of increased transmissibility + differential mixing.
But attributing the data entirely to increased transmissibility (i.e., assuming homogeneous mixing) likely overestimates B117 transmissibility.
But attributing the data entirely to increased transmissibility (i.e., assuming homogeneous mixing) likely overestimates B117 transmissibility.
I know the example presented here is simplistic, and I'm not suggesting that the rise of B117 is entirely due to differentials in mixing. It is likely that B117 is (at least somewhat) more transmissible.
But I do think we need more data on mixing before calling this case closed.
But I do think we need more data on mixing before calling this case closed.
Summary: Data from Denmark on B117 can be explained without invoking a dramatic increase in transmissibility.
But while data (and better models) continue to come in, our best defense against future increases in transmissibility is to keep levels of transmission low today.
But while data (and better models) continue to come in, our best defense against future increases in transmissibility is to keep levels of transmission low today.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


