
Why is fever considered to be ≥ 100.4 F?
A wonderful Tweetorial by @JennyShihMD, reviewed by @AvrahamCooperMD and @AdamRodmanMD.
A wonderful Tweetorial by @JennyShihMD, reviewed by @AvrahamCooperMD and @AdamRodmanMD.

100.4 comes from a single study in 1868 (archive.org/details/dasver…). Since then, multiple studies have refuted this, showing that fever on average can be as low as 99.5F (99th percentile of normal).
But the old definition has stuck. Let’s learn more about fevers in this 🧵.
But the old definition has stuck. Let’s learn more about fevers in this 🧵.

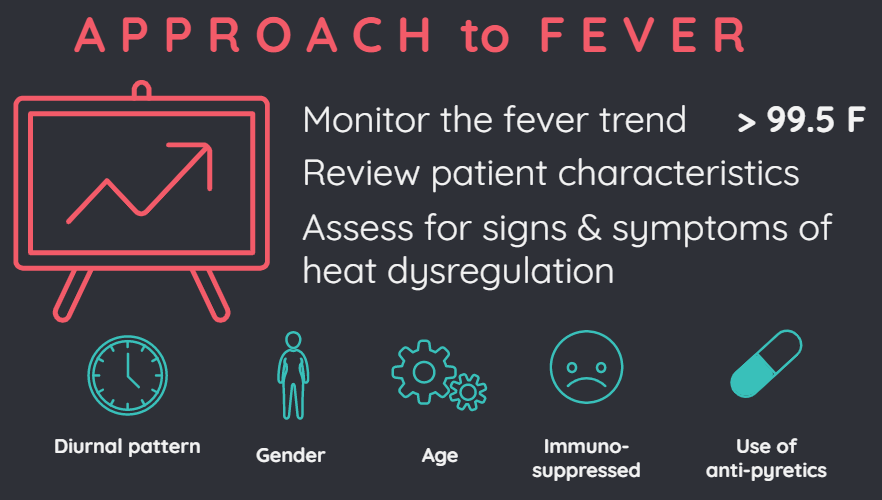
Trending the fever curve is more informative than a single measurement.
Body temperature varies by:
🕒 time of day;
⚥ gender; and
🎂 age.
Temperature is ⬇️in the AM and ⬆️in the late afternoon.
Women have ⬆️body temperature than men.
Older people have ⬇️temps than younger
Body temperature varies by:
🕒 time of day;
⚥ gender; and
🎂 age.
Temperature is ⬇️in the AM and ⬆️in the late afternoon.
Women have ⬆️body temperature than men.
Older people have ⬇️temps than younger

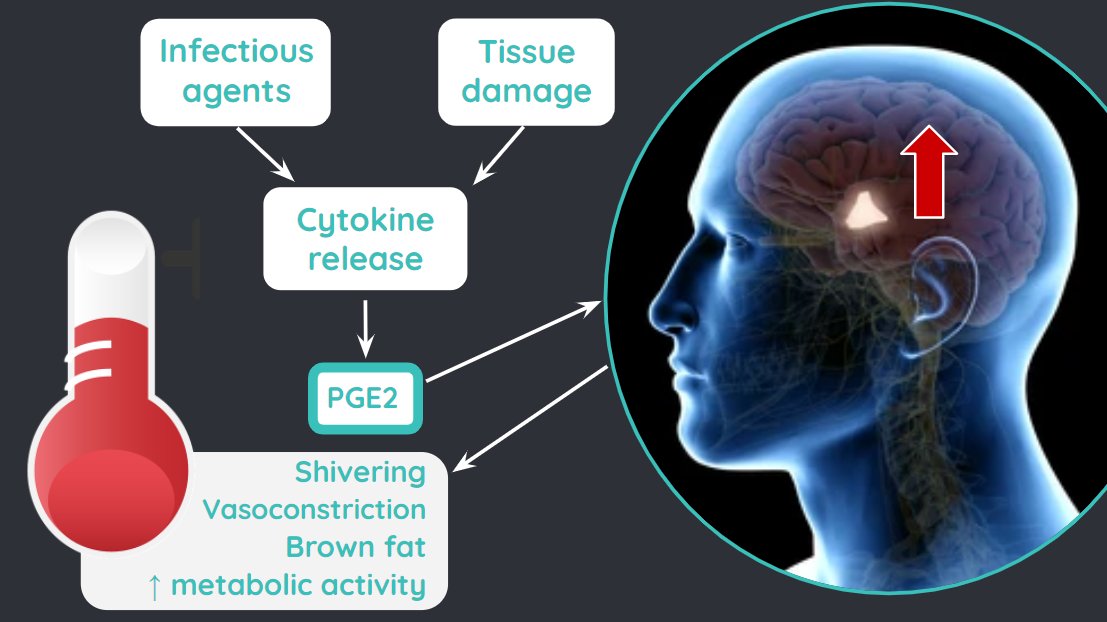
The hypothalamus is the body's thermoregulatory center. Fever occurs when the hypothalamic set point is increased due to high levels of prostaglandin E2 (PGE2). Tylenol and NSAIDs work by inhibiting synthesis of PGE2. (…-nature-com.ezp-prod1.hul.harvard.edu/articles/nri38…)
.@tony_breu has done a wonderful Tweetorial on the mechanism of night sweats (
https://twitter.com/tony_breu/status/1127262873577766912), and @AdamRodmanMD has explored the literature on fever cutoffs before (
https://twitter.com/AdamRodmanMD/status/1127935638685270016) so I want to do something a little bit different!
Time for a poll!
Should everyone with temperature 100.4F or higher be treated with acetaminophen? Please comment your thoughts!
Should everyone with temperature 100.4F or higher be treated with acetaminophen? Please comment your thoughts!
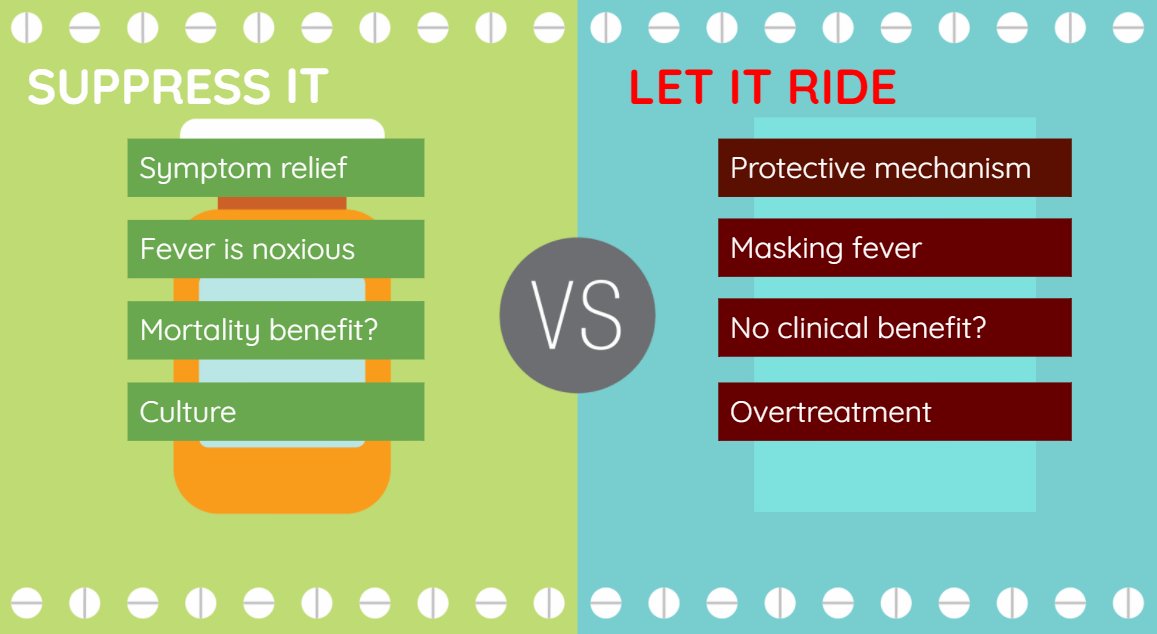
Treating fevers with antipyretics is controversial.
Arguments for treatment include symptom relief and that fevers itself are noxious. During fevers, there is increased oxygen demand, which may be harmful to those with cardiopulmonary limitations.
Arguments for treatment include symptom relief and that fevers itself are noxious. During fevers, there is increased oxygen demand, which may be harmful to those with cardiopulmonary limitations.
Fevers also can be harmful during hypoxic brain injury, ie. post cardiac arrest.
On the other hand, fevers can be a protective mechanism by stimulating the innate and adaptive immune responses to fight infection and inflammation. Antipyretics can mask fevers that can give us diagnostic clues. Lastly, some studies suggest no clinical benefit with acetaminophen
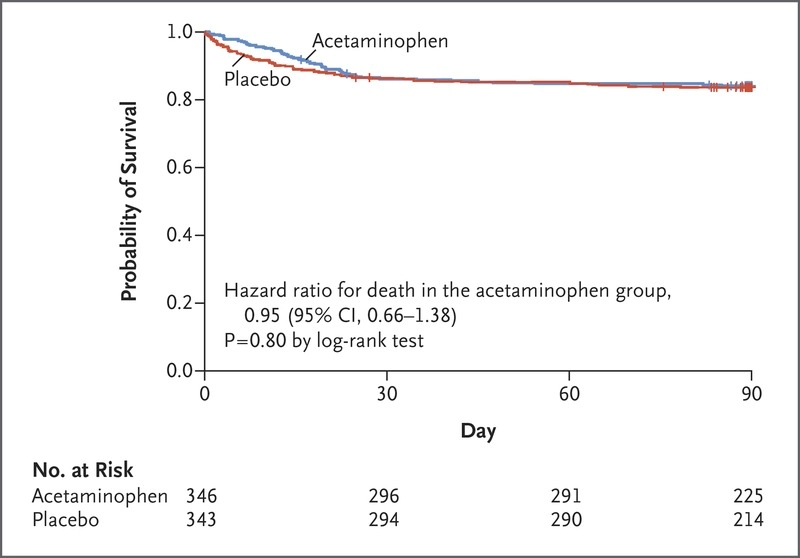
The “HEAT” trial found no differences in ICU free days and mortality when comparing standing tylenol with placebo in ICU patients with fevers and known/suspected infection. (pubmed.ncbi.nlm.nih.gov/26436473/)
What is my takeaway from all this?
1⃣ The definition of fever is outdated and inaccurate.
2⃣ Fever can be as low as ~99.5F based on recent studies.
3⃣ Trend the fever curve, rather than a single measurement.
4⃣ Every fever may not need to be treated with antipyretics.
1⃣ The definition of fever is outdated and inaccurate.
2⃣ Fever can be as low as ~99.5F based on recent studies.
3⃣ Trend the fever curve, rather than a single measurement.
4⃣ Every fever may not need to be treated with antipyretics.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



