
Let's do a new tutorial
GI-Bleeding for non-endoscopists
#MedTwitter #GITwitter #livertwitter #ICU #FOAMed
@stevenbollipo @drkeithsiau @ebtapper @jaumebosch9 @GI_Pearls @DrHarryThomas (these are endoscopists)
GI-Bleeding for non-endoscopists
#MedTwitter #GITwitter #livertwitter #ICU #FOAMed
@stevenbollipo @drkeithsiau @ebtapper @jaumebosch9 @GI_Pearls @DrHarryThomas (these are endoscopists)
First rule, stay cool
There are three different GI-bleeding locations:
upper (until suspensory muscle of duodenum)
middle
lower (starting from the coecum)
upper (until suspensory muscle of duodenum)
middle
lower (starting from the coecum)
Frequency:
upper>middle>lower
So, first gastroscopy before coloscopy
(exception: it is really clear like fifth times diverticle bleedings --> why did the patient receive no surgery?)
upper>middle>lower
So, first gastroscopy before coloscopy
(exception: it is really clear like fifth times diverticle bleedings --> why did the patient receive no surgery?)
One important differentiation:
upper GI-Bleeding
bleeding of varices vs. "usual" upper GI-Bleeding
upper GI-Bleeding
bleeding of varices vs. "usual" upper GI-Bleeding
First step is not the endoscopy!
But Basic management:
Anamnesis and physical examination:
Tumor? Cirrhosis? Medication(!)? History of bleeding?
What does the patient want? Palliative situation?
Anamnesis and physical examination:
Tumor? Cirrhosis? Medication(!)? History of bleeding?
What does the patient want? Palliative situation?
More basics:
Vitals, laboratory (Hb? coagulation parameters? Ca?, lactate).
Vitals, laboratory (Hb? coagulation parameters? Ca?, lactate).
More Basics
Stabilize the patient:
Give Volume
Get transfusion maybe (aim a Hb of 7mg/dl, but in heavy bleedings, aim higher, he'll hit the 7 or lower).
Beyond Basics: Intubation if GCP<9 or if he can puke the blood in the beam)
Give Volume
Get transfusion maybe (aim a Hb of 7mg/dl, but in heavy bleedings, aim higher, he'll hit the 7 or lower).
Beyond Basics: Intubation if GCP<9 or if he can puke the blood in the beam)
Stabilize the coagulation:
First with, guess it, basics:
Keep him warm >34°
ph>7.2
give Ca if ionized Ca<0.9 (Factor IV!)
Think about FFP (250 ml increase Quick about 6%)
and PPSB: 1 IE/kg increases Quick about 1%
Fibrinogen 2-4(-8g)
Individual concept
First with, guess it, basics:
Keep him warm >34°
ph>7.2
give Ca if ionized Ca<0.9 (Factor IV!)
Think about FFP (250 ml increase Quick about 6%)
and PPSB: 1 IE/kg increases Quick about 1%
Fibrinogen 2-4(-8g)
Individual concept
Hint:
If a patient bleeds again and again, diffuse, you don't find anything. Check Factor XIII. Decrease of it can be the cause. Substitute.
If a patient bleeds again and again, diffuse, you don't find anything. Check Factor XIII. Decrease of it can be the cause. Substitute.
Don't let him do this:
But give parenteral nutrition to cirrhosis patients (they loose muscles fast).
Vomiting red blood and black stool --> upper GI-bleeding
bloody stool --> lower GI Bleeding
BUT: Blood is like laxative --> bloody stool can be upper GI-bleeding, too.
bloody stool --> lower GI Bleeding
BUT: Blood is like laxative --> bloody stool can be upper GI-bleeding, too.
Upper GI-Bleeding:
Forrest I a (Spurting hemorrhage)
Forrest I b (Oozing hemorrhage)
Forrest II a (Non bleeding Visible vessel)
Forrest II b (Adherent clot)
Forrest II c (Flat pigmented haematin (coffee ground base) on ulcer base)
and
Forrest I a (Spurting hemorrhage)
Forrest I b (Oozing hemorrhage)
Forrest II a (Non bleeding Visible vessel)
Forrest II b (Adherent clot)
Forrest II c (Flat pigmented haematin (coffee ground base) on ulcer base)
and
Forrest III (Lesions without signs of recent hemorrhage or fibrin-covered clean ulcer base)
Forrest I b --> highest risk of rebreeding!
Forrest I b --> highest risk of rebreeding!
Now, you have done something. Actually a lot.
Call the endoscopist and make a concept.
Call the endoscopist and make a concept.
While you are doing this give a PPI:
8-10 mg/h Pantozol
3x40 mg Bolus or continously 240mg/24 h
8-10 mg/h Pantozol
3x40 mg Bolus or continously 240mg/24 h
Before gastroscopy give erythrmycin 250 mg i. v. (30-120 min before). I suggest 30min, because it will take longer anyway.
Special case: Varices bleeding:
If you think, the patient has it:
-still give PPI, stop when varices bleeding is proven
- give antibiotics! Ceftriaxon 2 g (over 5-7 day, if patient is stabile, give it p. o. e.g. (amonicillin/clavulan acid)
-give something vasoactive!
If you think, the patient has it:
-still give PPI, stop when varices bleeding is proven
- give antibiotics! Ceftriaxon 2 g (over 5-7 day, if patient is stabile, give it p. o. e.g. (amonicillin/clavulan acid)
-give something vasoactive!
Vasactive would be:
Terlipressin: 2 mg i. v. every 4 hours
Somatostatin: 250 mikrogramm bolus, then 250 mikrogramm/hour
Octreotid: 50 mikrogramm bolus, then 50 mikrogramm/hour
I do it so: Somatostatin: 3 mg in 36 ml NaCl; Bolus 3ml
dann 3 ml/h continously
Terlipressin: 2 mg i. v. every 4 hours
Somatostatin: 250 mikrogramm bolus, then 250 mikrogramm/hour
Octreotid: 50 mikrogramm bolus, then 50 mikrogramm/hour
I do it so: Somatostatin: 3 mg in 36 ml NaCl; Bolus 3ml
dann 3 ml/h continously
Avoid PPIs in Cirrhosis patients:
Some people like to give them, when ligatures are very down. Then: prefer esomeprazole, only for a short time
Some people like to give them, when ligatures are very down. Then: prefer esomeprazole, only for a short time
If you (or the endoscopist) cannot stop the bleeding from varices:
TIPS ----> emergency!
TIPS ----> emergency!
After varices bleeding:
secondary prophylaxis with non-selective beta-blocker
Propanolol or better Carvedilol (e.g. 12,5mg 1-0-0 or 6,25 mg 1-0-1)
secondary prophylaxis with non-selective beta-blocker
Propanolol or better Carvedilol (e.g. 12,5mg 1-0-0 or 6,25 mg 1-0-1)
If you don't find the bleeding source up go
down
down
down
down
down
down
down
down
If there is no source neither
Options:
Capsule endoscopy
double ballon enteroscopy
spiral endoscopy
Angio-CT (you only see something there, if there is active bleeding)
Capsule endoscopy
double ballon enteroscopy
spiral endoscopy
Angio-CT (you only see something there, if there is active bleeding)
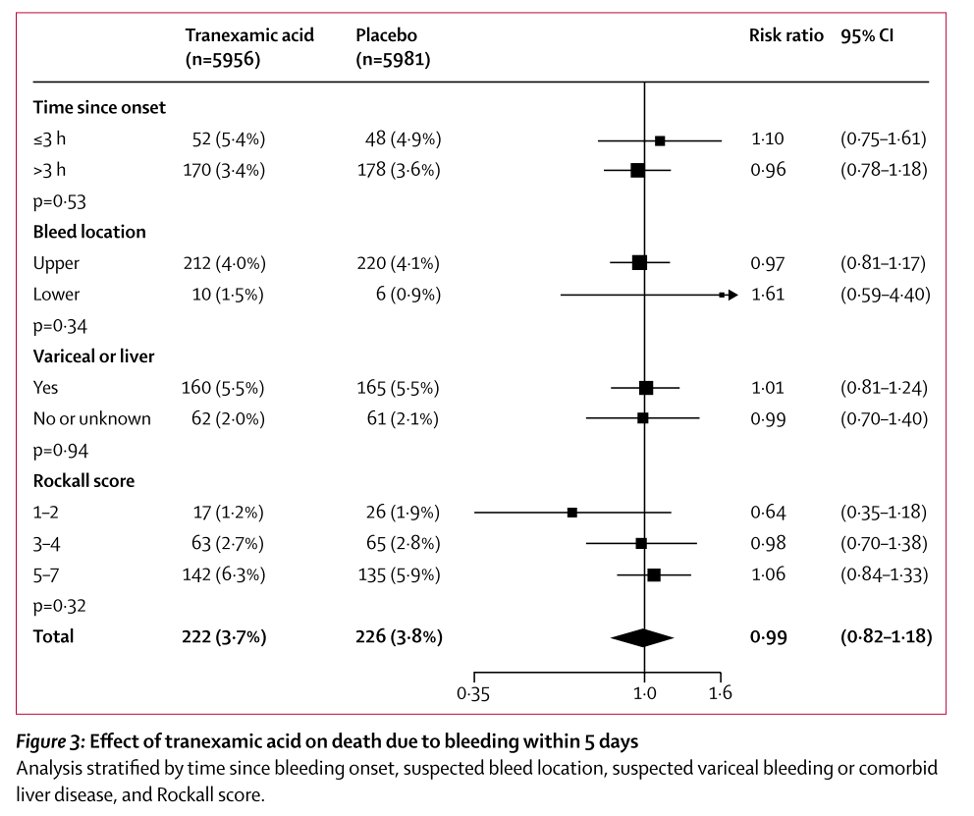
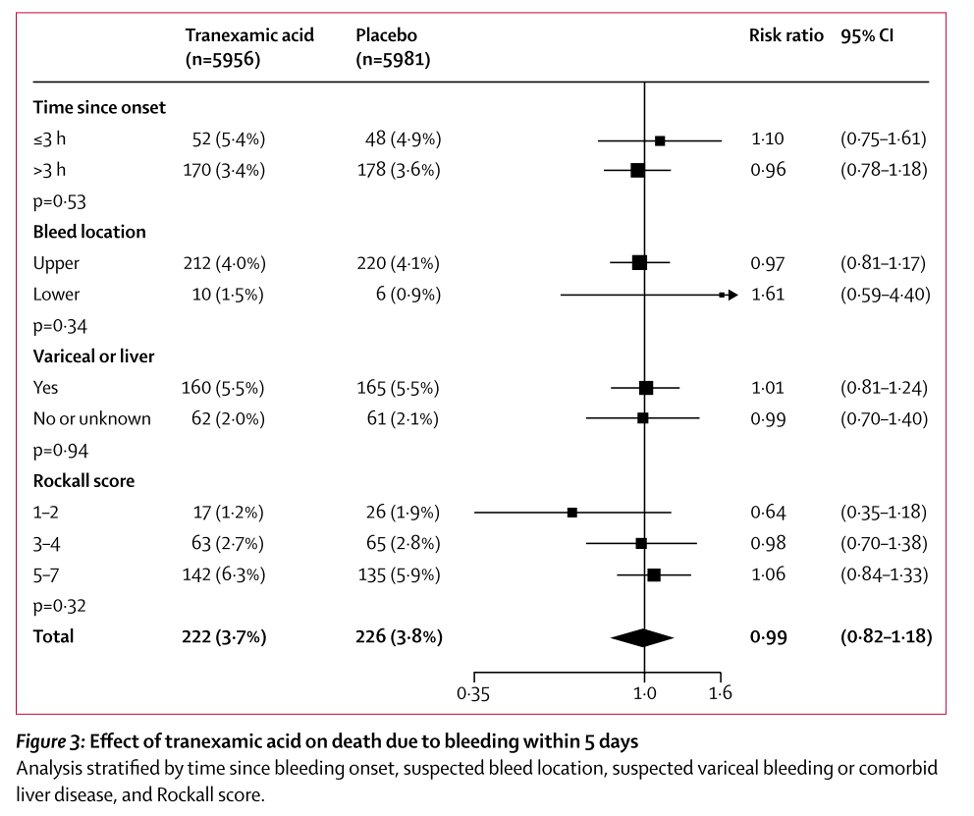
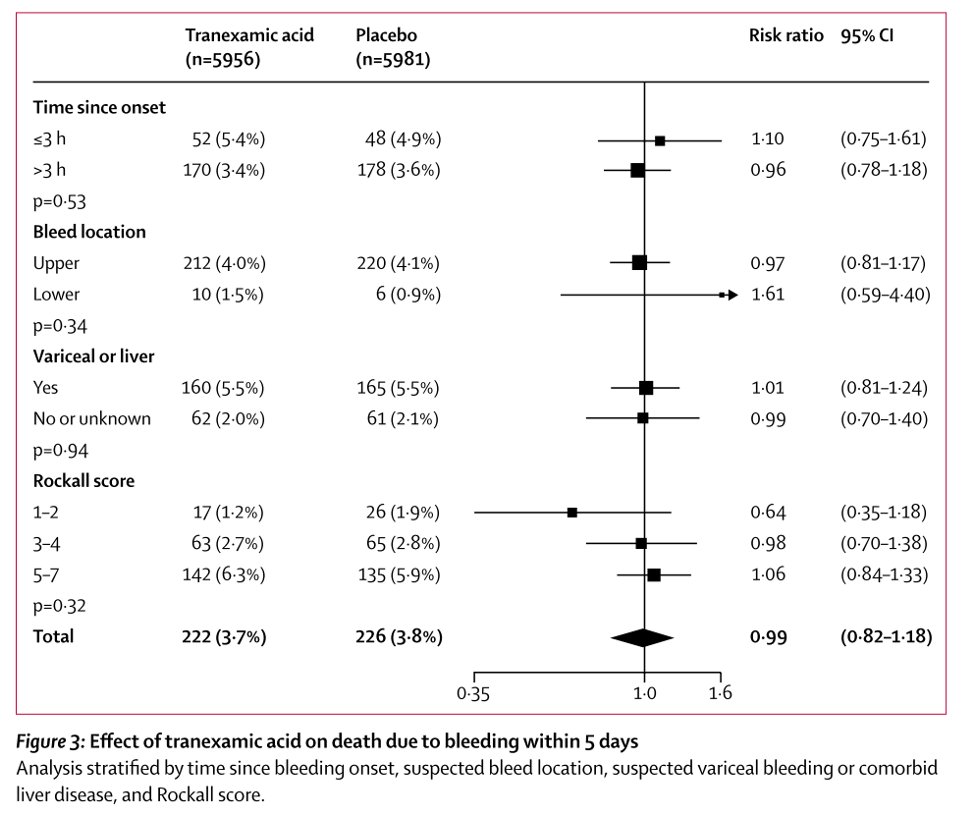
No tranexam acid: not less rebleedings but more thrombosis 
This is from:
Dieulafoy Lesions:
If possible: Doppler endoscopic probe (DEP)–guided therapy
Rebleeding within 30 days occurred in 11% of those treated with DEP-guided endoscopic therapy compared with 33% of those receiving visually-guided hemostasis.
If possible: Doppler endoscopic probe (DEP)–guided therapy
Rebleeding within 30 days occurred in 11% of those treated with DEP-guided endoscopic therapy compared with 33% of those receiving visually-guided hemostasis.
Source:
(NEJM JW Gastroenterol Oct 2020 and Clin Gastroenterol Hepatol 2020 Aug 20; [e-pub])
(NEJM JW Gastroenterol Oct 2020 and Clin Gastroenterol Hepatol 2020 Aug 20; [e-pub])
I am from Germany.
NICE guidelines say: First Angio-CT, then, radiological intervention or colposcopy. I don't think that helps a lot, because there have to be enough bleeding to see something in angio ct (what do you think @drkeithsiau ?)
NICE guidelines say: First Angio-CT, then, radiological intervention or colposcopy. I don't think that helps a lot, because there have to be enough bleeding to see something in angio ct (what do you think @drkeithsiau ?)
Anamnesis and examination --> patient's will --> stabilization --> gastroscopy --> colposcopy --> rethinking (middle GI bleeding? Angio-CT)
Thank you for your attention.
Feel free to comment, ask, discuss, insult, retweet or ignore.
Feel free to comment, ask, discuss, insult, retweet or ignore.
How could I forget? @DeMadaria
Vasactive would be:
Terlipressin: 2 mg i. v. every 4 hours
Somatostatin: 250 mikrogramm bolus, then 250 mikrogramm/hour
Octreotid: 50 mikrogramm bolus, then 50 mikrogramm/hour
I do it so: Somatostatin: 3 mg in 36 ml NaCl; Bolus 3ml
dann 3 ml/h continously
Terlipressin: 2 mg i. v. every 4 hours
Somatostatin: 250 mikrogramm bolus, then 250 mikrogramm/hour
Octreotid: 50 mikrogramm bolus, then 50 mikrogramm/hour
I do it so: Somatostatin: 3 mg in 36 ml NaCl; Bolus 3ml
dann 3 ml/h continously
Avoid PPIs in Cirrhosis patients:
Some people like to give them, when ligatures are very down. Then: prefer esomeprazole, only for a short time
Some people like to give them, when ligatures are very down. Then: prefer esomeprazole, only for a short time
If you (or the endoscopist) cannot stop the bleeding from varices:
TIPS ----> emergency!
TIPS ----> emergency!
After varices bleeding:
secondary prophylaxis with non-selective beta-blocker
Propanolol or better Carvedilol (e.g. 12,5mg 1-0-0 or 6,25 mg 1-0-1)
secondary prophylaxis with non-selective beta-blocker
Propanolol or better Carvedilol (e.g. 12,5mg 1-0-0 or 6,25 mg 1-0-1)
If you don't find the bleeding source up go
down
down
down
down
down
down
down
down
If there is no source neither
Options:
Capsule endoscopy
double ballon enteroscopy
spiral endoscopy
Angio-CT (you only see something there, if there is active bleeding)
Capsule endoscopy
double ballon enteroscopy
spiral endoscopy
Angio-CT (you only see something there, if there is active bleeding)
No tranexam acid: not less rebleedings but more thrombosis
No tranexam acid: not less rebleedings but more thrombosis
Source:

Dieulafoy Lesions:
If possible: Doppler endoscopic probe (DEP)–guided therapy
Rebleeding within 30 days occurred in 11% of those treated with DEP-guided endoscopic therapy compared with 33% of those receiving visually-guided hemostasis.
If possible: Doppler endoscopic probe (DEP)–guided therapy
Rebleeding within 30 days occurred in 11% of those treated with DEP-guided endoscopic therapy compared with 33% of those receiving visually-guided hemostasis.
Source:
(NEJM JW Gastroenterol Oct 2020 and Clin Gastroenterol Hepatol 2020 Aug 20; [e-pub])
(NEJM JW Gastroenterol Oct 2020 and Clin Gastroenterol Hepatol 2020 Aug 20; [e-pub])
I am from Germany.
NICE guidelines say: First Angio-CT, then, radiological intervention or colposcopy. I don't think that helps a lot, because there have to be enough bleeding to see something in angio ct (what do you think
@drkeithsiau ?)
NICE guidelines say: First Angio-CT, then, radiological intervention or colposcopy. I don't think that helps a lot, because there have to be enough bleeding to see something in angio ct (what do you think
@drkeithsiau ?)
By the way. How could I forget?
@DeMadaria
@DeMadaria
Thank you very much for your attention.
Feel free to comment, ask, discuss, insult, retweet or ignore.
Feel free to comment, ask, discuss, insult, retweet or ignore.
I am sorry. I messed a little up. This is the complete thread. Insult, please.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


