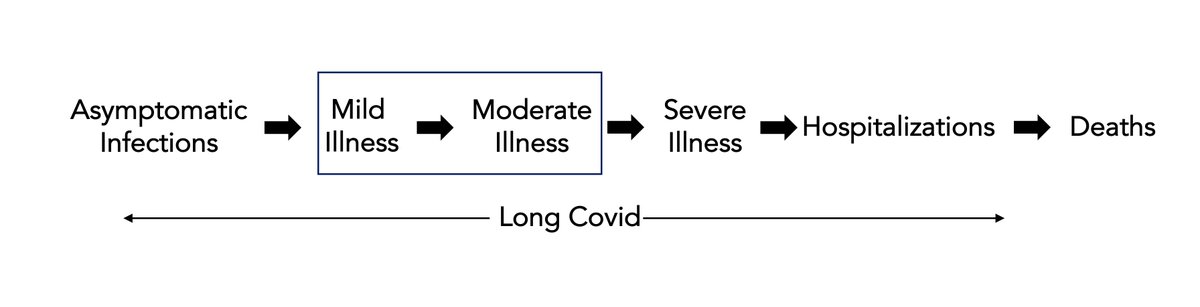
The spectrum of covid illness and effect of the vaccines in clinical trials
1. The trials were designed and powered for protection from mild to moderate illness. Not severe infections. Not asymptomatic infections. Not hospitalizations or deaths. Not #LongCovid.
1. The trials were designed and powered for protection from mild to moderate illness. Not severe infections. Not asymptomatic infections. Not hospitalizations or deaths. Not #LongCovid.
2. The Table summarizes the data to point out how few severe endpoints occurred. The largest N of endpoints was in the J&J trial and <10% fell into the "severe" category. All together for over 152,000 participants, <100 severe endpoints.

3. We registered concern last fall about this matter, that there will be inadequate events/statistical power to judge severe infections and outcomes nytimes.com/2020/09/22/opi…

4. The different trials in different countries makes same comparisons difficult, but we can adjust for the D614G strain: the efficacy for mRNA vaccines was 95%, Sputnik V 91% and J&J 72%. A > 20 point percent drop-off.
@maggiekb1 has a very good 🧵today
@maggiekb1 has a very good 🧵today
https://twitter.com/maggiekb1/status/1367870071993929735
5. What does this mean for asymptomatic infections?
If mild infections are suppressed more, then you might expect the same for the carrier state. Proper studies with very frequent assessment for shedding, viral load are pending (we don't know yet)
If mild infections are suppressed more, then you might expect the same for the carrier state. Proper studies with very frequent assessment for shedding, viral load are pending (we don't know yet)
6. What does this mean for #LongCovid?
If you don't suppress mild and moderate infections well, which represent the largest fraction of LongCovid, there will be a gap in impact of a vaccine. Not what the trials were designed for. An inference.
If you don't suppress mild and moderate infections well, which represent the largest fraction of LongCovid, there will be a gap in impact of a vaccine. Not what the trials were designed for. An inference.

7. From the clinical trial data, to say there is equivalent efficacy for J&J is incorrect; the assertion is based on a very limited number of "severe" events, a small fraction (<10%) of endpoints. Vaccines have potential impact across the full clinical spectrum.
8. Good discussion on vaccine efficacy @NYTScience nytimes.com/interactive/20… by @carlzimmer @collinskeith but it oversteps on hospitalizations and deaths, for which there are not enough events and this was not the 1° endpoint

9. Here @DLeonhardt reviews the vaccine efficacy and particularly the concern about J&J 's. nytimes.com/2021/03/04/bri…
He discounts the importance of mild infections (should be mild and moderate), the primary endpoint of the trials.
He discounts the importance of mild infections (should be mild and moderate), the primary endpoint of the trials.

10. In the same article it is stated: "The number that we should all truly care about is what are the chances I'm going to get this thing and get really sick or die. There is essentially no chance you will die of Covid, which is breathtaking"—@Bob_Wachter
11. That unfortunately isn't certain since the trials were woefully underpowered for severe illness, hospitalizations and deaths. And mild/moderate infections do have implications (spread, #LongCovid) which can't be ignored. Things to keep in mind for judging efficacy
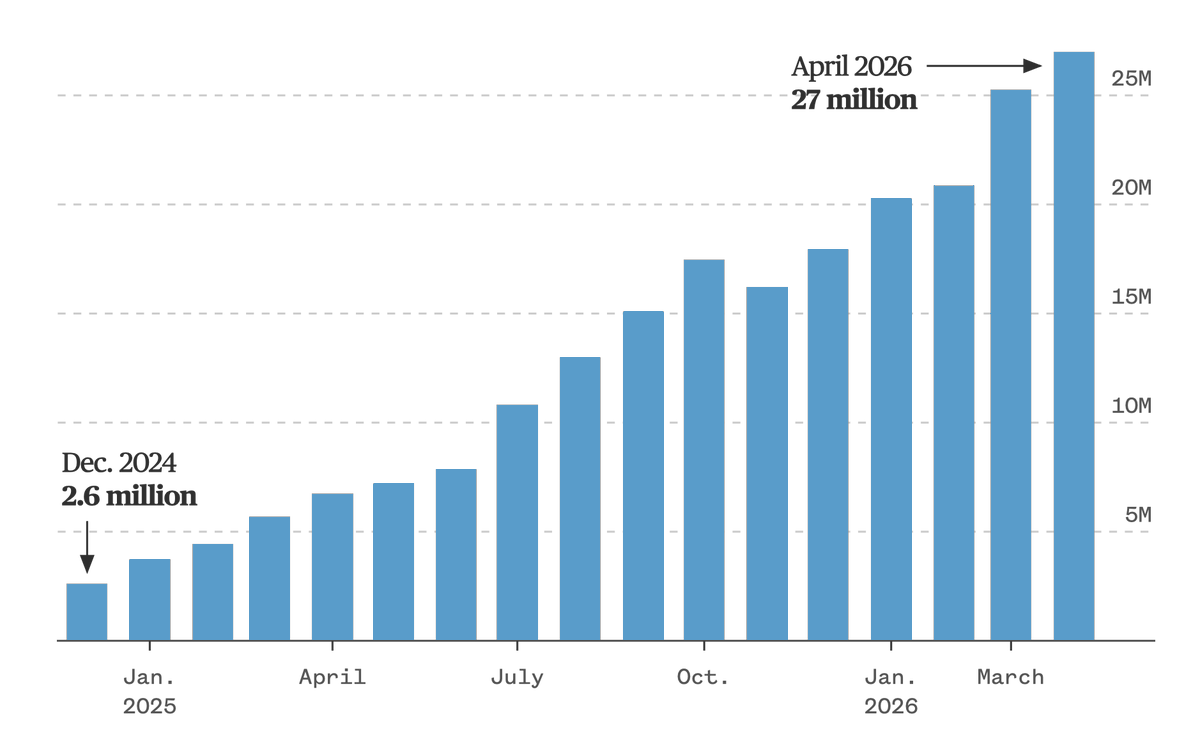
12. The real proof of vaccine protection from severe covid-19, deaths and hospitalizations comes from millions of people w/ real world evidence (unfortunately, not RCTs). There's no shortage of that emerging now from Israel, the UK, and US nursing homes
• • •
Missing some Tweet in this thread? You can try to
force a refresh