
COVID on the brain 🧠
Stroke like brain injury can be a life altering complication of SARS-COV-2 infection
Let's see how often is happens, what it looks like, and why.
A retrospective study was done in my own hospital trust :)
1/
Stroke like brain injury can be a life altering complication of SARS-COV-2 infection
Let's see how often is happens, what it looks like, and why.
A retrospective study was done in my own hospital trust :)
1/

3,403 PCR+ COVID inpatients between March and May 2020
167 had neurological symptoms warranting neuroimaging
38 revealed vascular (ischemic or haemorrhagic) abnormality = 1.12% of total C19 inpatients
Mean age 59.7
Onset of neuro symptoms mean 10.1 days from admission
2/
167 had neurological symptoms warranting neuroimaging
38 revealed vascular (ischemic or haemorrhagic) abnormality = 1.12% of total C19 inpatients
Mean age 59.7
Onset of neuro symptoms mean 10.1 days from admission
2/

Even w/out COVID, many patients admitted for other reasons have strokes. However, in this COVID patient cohort when age adjusted the rate is ~5x ⬆️
87 vs 16 per 1000 hospitalised inpatients annualised rate
3/
87 vs 16 per 1000 hospitalised inpatients annualised rate
3/
What do these look like on brain MRI:
- microhaemorrhages (commonest)
- watershed white matter hyperintensities
- susceptibility changes on SWI in superficial veins
- hypoxic-ischaemic changes
4/
- microhaemorrhages (commonest)
- watershed white matter hyperintensities
- susceptibility changes on SWI in superficial veins
- hypoxic-ischaemic changes
4/




MRI features continued:
- parenchymal and subarachnoid haemorrhage
- acute and subacute infarct
- acute haemorrhagic necrotising encephalopathy (PRES)
- ADEM like changes
5/
- parenchymal and subarachnoid haemorrhage
- acute and subacute infarct
- acute haemorrhagic necrotising encephalopathy (PRES)
- ADEM like changes
5/


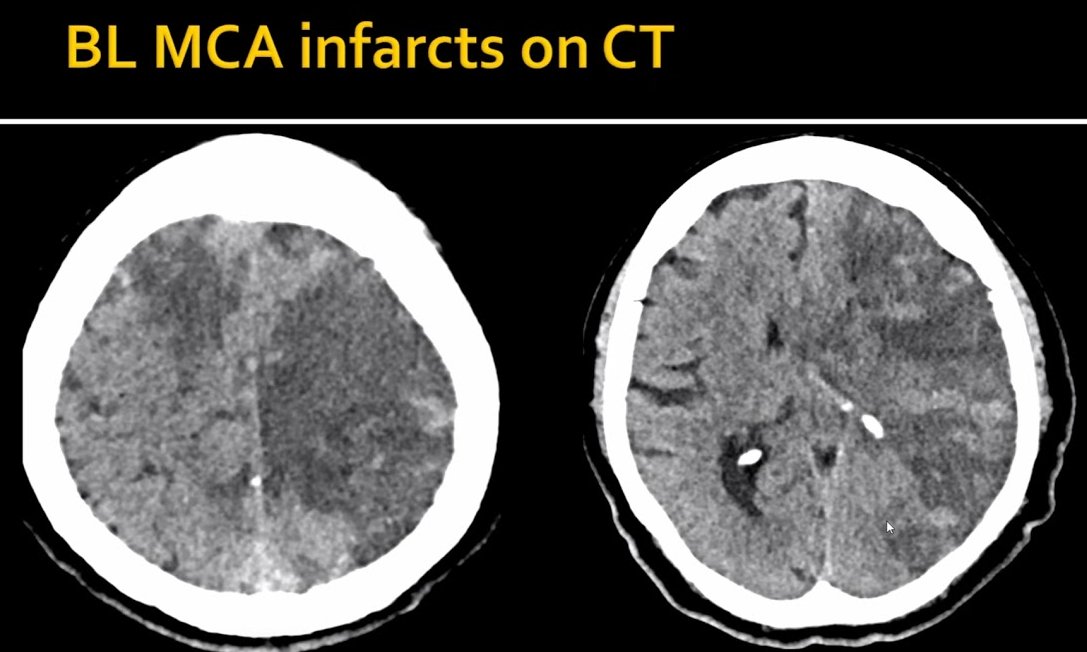
CT findings:
- Acute and subacute infarcts
- basal ganglia haemorrhage
- subarachnoid haemorrhage
6/
- Acute and subacute infarcts
- basal ganglia haemorrhage
- subarachnoid haemorrhage
6/

Mechanism:
- pro-inflammatory cytokine storm (IL-6, TNF-a)
- blood-brain and blood-CSF barrier dysfunction
- direct neuroinflammation
-micro vascular disruption of endothelium = extravasation of RBC/microhaemorrhages
- inflammatory neutrophil extracellular trap= thrombus
7/
- pro-inflammatory cytokine storm (IL-6, TNF-a)
- blood-brain and blood-CSF barrier dysfunction
- direct neuroinflammation
-micro vascular disruption of endothelium = extravasation of RBC/microhaemorrhages
- inflammatory neutrophil extracellular trap= thrombus
7/

Although our hospital did not see a case of central venous sinus thrombosis (CVST), there is evidence of association/higher event rate with COVID👇
(same pathophysiology as presented above)
Typical background rate is 2-15 per million per year.
8/
strokejournal.org/article/S1052-…
(same pathophysiology as presented above)
Typical background rate is 2-15 per million per year.
8/
strokejournal.org/article/S1052-…
So in a country with high COVID prevalence the expectation will be CVST rate will be higher than typical year. Temporal association with a vax may be incidental to recent or new infection etc.
So more care than usual has to be taken to disentangle
9/
So more care than usual has to be taken to disentangle
9/
https://twitter.com/olivernmoody/status/1371526339002515463
Likely preventing ~120 severe hospitalised COVID cases stops 1 cerebrovascular event.
V consequential as can be permanently debilitating, life shortening or threatening.
Even compared to 'possible' CVST 🇩🇪 AZ vax saves an order of magnitude more from neurological events
V consequential as can be permanently debilitating, life shortening or threatening.
Even compared to 'possible' CVST 🇩🇪 AZ vax saves an order of magnitude more from neurological events
• • •
Missing some Tweet in this thread? You can try to
force a refresh






