
1/
First of 2 tweets! #GalactoMagic
50F w/ EtOH cirrhosis & DM presents to ED w/ AMS & decreased UOP. She is febrile & hypotensive
She is started on vasopressors & CVVHD via central lines in the ICU
Due to concern for SBP, she is started on ceftriaxone
First of 2 tweets! #GalactoMagic
50F w/ EtOH cirrhosis & DM presents to ED w/ AMS & decreased UOP. She is febrile & hypotensive
She is started on vasopressors & CVVHD via central lines in the ICU
Due to concern for SBP, she is started on ceftriaxone
2/
Initial blood & ascites cultures show no growth. She remains critically ill for 7 days and still having fevers
In addition to blood cultures, which of the following is the next best test to order?
Initial blood & ascites cultures show no growth. She remains critically ill for 7 days and still having fevers
In addition to blood cultures, which of the following is the next best test to order?
1/13
Answer: Serum BDG
You have suspicion for invasive candidiasis given the RF of cirrhosis, critical illness in ICU w/ central lines, dialysis, & broad-spectrum antibiotics (see other RF in table)
Answer: Serum BDG
You have suspicion for invasive candidiasis given the RF of cirrhosis, critical illness in ICU w/ central lines, dialysis, & broad-spectrum antibiotics (see other RF in table)

2/
Others (@gayathri25788 & @fernandbteich) have alluded to crypto being a possibility
Yes, that is very true (hence why it wasn’t listed as an option here)
For a dive into cryptococcosis & cirrhosis, please review this question and thread
Others (@gayathri25788 & @fernandbteich) have alluded to crypto being a possibility
Yes, that is very true (hence why it wasn’t listed as an option here)
For a dive into cryptococcosis & cirrhosis, please review this question and thread
https://twitter.com/FilaMentor/status/1361726736078004224?s=20
3/
Fungal blood cx are rarely indicated
Providers should focus on collecting adequate # of standard blood culture bottles (2) & blood volume (5-10cc/bottle)
Fungal blood cx may be used for suspected disseminated infection from:
🌞Blasto
🌞Cocci
🌞Histo
🌞Malassezia (RF: TPN)
Fungal blood cx are rarely indicated
Providers should focus on collecting adequate # of standard blood culture bottles (2) & blood volume (5-10cc/bottle)
Fungal blood cx may be used for suspected disseminated infection from:
🌞Blasto
🌞Cocci
🌞Histo
🌞Malassezia (RF: TPN)
4/
For some great thoughts on fungal blood cultures, please see tweets from:
@KatesOlivia
&
@IdVilchez
For some great thoughts on fungal blood cultures, please see tweets from:
@KatesOlivia
https://twitter.com/KatesOlivia/status/1372591680918974467?s=20
&
@IdVilchez
https://twitter.com/IdVilchez/status/1372595402797506562?s=20
5/
In diagnosing invasive candidiasis, there are 3 entities that we consider:
⚡️Group 1- candidemia without deep-seated candidiasis
⚡️Group 2- candidemia with deep-seated candidiasis
⚡️Group 3- deep-seated candidiasis without candidemia
In diagnosing invasive candidiasis, there are 3 entities that we consider:
⚡️Group 1- candidemia without deep-seated candidiasis
⚡️Group 2- candidemia with deep-seated candidiasis
⚡️Group 3- deep-seated candidiasis without candidemia
6/
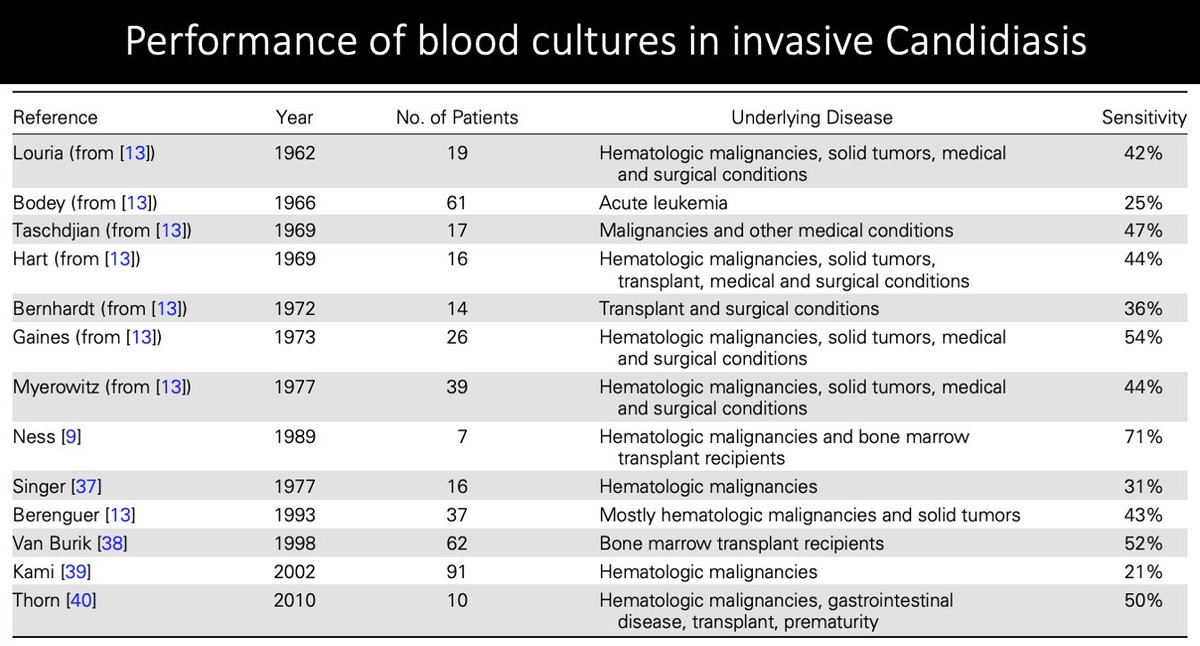
In studies of autopsy-proven invasive candidiasis, sens of blood cx ranged from 21-71%
This range applies to pts who were likely candidemic at some point
Patients in Group 2 were likely candidemic at one time, but may not have been candidemic at the time blood cx were drawn
In studies of autopsy-proven invasive candidiasis, sens of blood cx ranged from 21-71%
This range applies to pts who were likely candidemic at some point
Patients in Group 2 were likely candidemic at one time, but may not have been candidemic at the time blood cx were drawn
7/
If we look at just Group 1 (candidemia w/o deep-seated), sensitivity increases to 63-83%!
🌑Below is a summary of autopsy-proven invasive candidiasis
pubmed.ncbi.nlm.nih.gov/23315320/
If we look at just Group 1 (candidemia w/o deep-seated), sensitivity increases to 63-83%!
🌑Below is a summary of autopsy-proven invasive candidiasis
pubmed.ncbi.nlm.nih.gov/23315320/
8/
Now, shifting to candidemia...
The median time to blood culture positivity is 2-3 days (perhaps better than the turnaround time for BDG at some hospitals)
We have to think about the RFs in Tweet 1 in trying to identify candidemia, especially if a patient is not improving
Now, shifting to candidemia...
The median time to blood culture positivity is 2-3 days (perhaps better than the turnaround time for BDG at some hospitals)
We have to think about the RFs in Tweet 1 in trying to identify candidemia, especially if a patient is not improving
9/
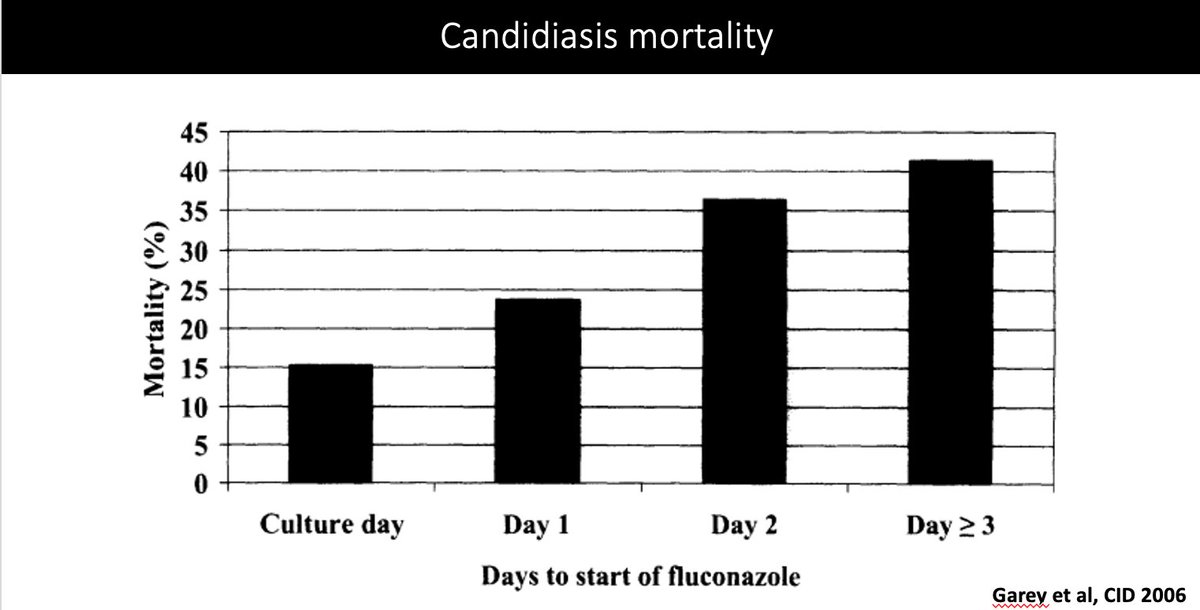
Why is identifying candidemia important?
Retrospective study across 4 sites looked at 230 pts w/ candidemia & time to fluconazole start
At Day 0, mortality was 15%
⭐️For each day of treatment delay, you have ⬆️mortality (more than doubles by Day 2)
pubmed.ncbi.nlm.nih.gov/16758414/
Why is identifying candidemia important?
Retrospective study across 4 sites looked at 230 pts w/ candidemia & time to fluconazole start
At Day 0, mortality was 15%
⭐️For each day of treatment delay, you have ⬆️mortality (more than doubles by Day 2)
pubmed.ncbi.nlm.nih.gov/16758414/
10/
What about BDG testing for invasive candidiasis in the ICU?
💫BDG and Candida studies differ with respect to patient population, risk factors, & timing of BDG testing
⭐️Generally, they suggest a NPV > 90% & PPV < 70%
academic.oup.com/cid/article/72…
What about BDG testing for invasive candidiasis in the ICU?
💫BDG and Candida studies differ with respect to patient population, risk factors, & timing of BDG testing
⭐️Generally, they suggest a NPV > 90% & PPV < 70%
academic.oup.com/cid/article/72…
11/
Since NPV is high, a negative BDG can be used to hold or d/c antifungals
+BDG prompting antifungals is less clear 2/2 lower PPV, but can be helpful in high-risk pts
(abd surgery, GI perf, hepatobiliary anastomotic leakage; necrotizing pancreatitis)
academic.oup.com/cid/article/72…
Since NPV is high, a negative BDG can be used to hold or d/c antifungals
+BDG prompting antifungals is less clear 2/2 lower PPV, but can be helpful in high-risk pts
(abd surgery, GI perf, hepatobiliary anastomotic leakage; necrotizing pancreatitis)
academic.oup.com/cid/article/72…
12/
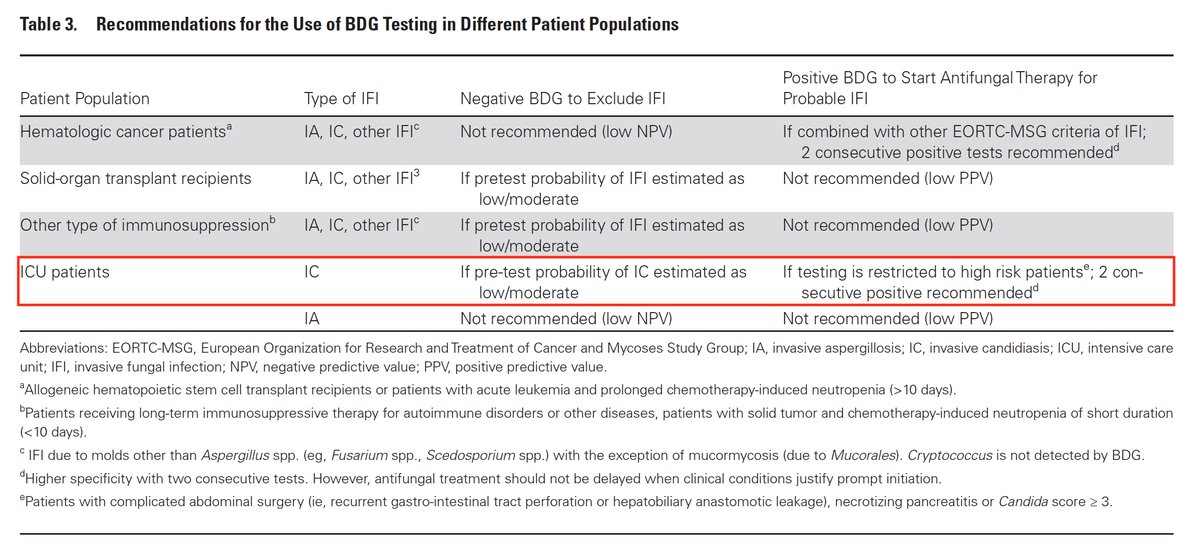
A group from European Organization for Research & Treatment of Cancer & Mycoses Study Group Education & Research Consortium (EORTC/MSGERC) reviewed the updated fungal guidelines, specifically looking at BDG
In red is the BDG rec for Candida in ICU
academic.oup.com/cid/article/72…
A group from European Organization for Research & Treatment of Cancer & Mycoses Study Group Education & Research Consortium (EORTC/MSGERC) reviewed the updated fungal guidelines, specifically looking at BDG
In red is the BDG rec for Candida in ICU
academic.oup.com/cid/article/72…
13/
Due to "limited sens & spec, utility of serum BDG differs by pt population at risk of IFI"
"Prevalence of IFI in specific populations & pre-test probability of IFI in pts should be taken into account when interpreting negative & positive results"
academic.oup.com/cid/article/72…
Due to "limited sens & spec, utility of serum BDG differs by pt population at risk of IFI"
"Prevalence of IFI in specific populations & pre-test probability of IFI in pts should be taken into account when interpreting negative & positive results"
academic.oup.com/cid/article/72…
• • •
Missing some Tweet in this thread? You can try to
force a refresh



