
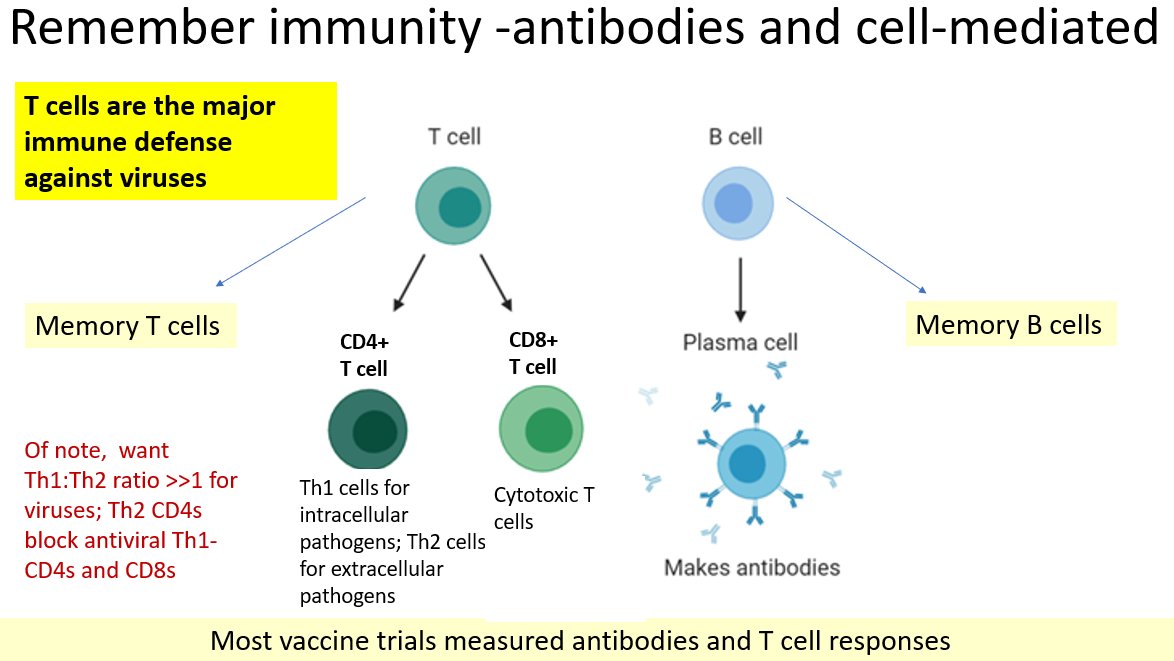
Wanted to drill down a bit more about the importance of the T-cell response to SARS-CoV-2 to give you more reassurance of enduring protection from vaccines (even against variants). Technical article here but CD4/CD8 cells have role in both acute infection cell.com/cell/pdf/S0092… 
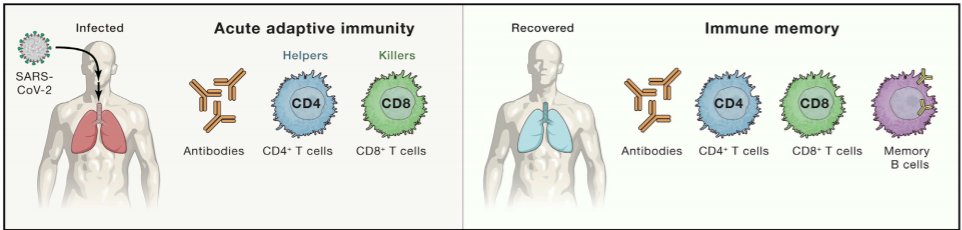
But, importantly, in recovered infection to give you durable immunity, along with memory B cells. Latter simulated by vaccine-induced immunity (you didn't get acute infection, you stimulate the immune response so that you can't get infected if you encounter virus). If you
just measure antibodies, you are measuring "tip of iceberg" in terms of your immune response to natural infection or vaccination so always ask - what about T cell responses to either? (and eventually, memory B cells too which give you long durable immunity). In fact, authors
compare just considering antibodies analogous to blindfolded person with elephant. CD4+ cell responses are more prominent than CD8+ cell responses with SARS-CoV-2 (see this paper) & have been associated with control of COVID-19. "Notably,
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
"SARS-CoV-2-specific CD4+ T cells had the strongest association with lessened COVID-19 disease severity, compared with antibodies and CD8+ T cells" (paper here). In fact, another paper (next tweet) shows rapid induction of CD4 associated with mild
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
disease & rapid clearance of virus. So, what about with vaccines? Well, all of them rapidly induce SARS-CoV-2 specific CD4 cells although closer inspection of phase I/II trials of candidates today show that Moderna does not induce CD8 cells as well
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
and Novavax vaccine press release only commented on strong CD4 cell response and didn't mention CD8 response- so refined table further here. So, we have already commented in previous thread that 1) AstraZeneca vaccine in S. Africa trial paper induced strong CD4/CD8 responses to

specific epitopes (bits) of the spike protein. And "of 87 spike-specific antigens [T cell epitopes] identified by the sequencing, 75 remained unaffected by the B.1.351 mutations." So, this probably explains why AZ is doing such a good job in protecting against severe disease in
in UK (and likely would protect against severe disease against S. Africa variant B.1.351 although trial not allowed to continue). And these strong and very in-breadth T cell responses with the vaccines likely explain the incredible protection against severe disease; those T cell
responses are unperturbed by variants since they form responses to so many parts of the spike protein that a few bits of the spike protein having mutations doesn't affect their ability to attack the virus (variant or other) if they see it. See this article researchsquare.com/article/rs-226…
and this one too to see the in-breadth T-cell response from vaccination against variants. A recent summary somewhere said "no one but scientists should be thinking about variants" & I agree that a general public focus on them detracts from realizing how
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
amazing these vaccines are. Influenza has a massive animal reservoir (swine, pigs, duck, birds, waterfowl where mutations are ongoing) in close contact with humans. Once COVID controlled in humans with regular vaccination, will become rare like other vaccine preventable diseases.
Want to add to this thread on T cells with another great paper showing how in-breadth your T cell response across the SPIKE PROTEIN is (e.g. cellular response that will be induced by vaccines). 57 T-cell epitopes conserved across geographic viral variants
jvi.asm.org/content/95/6/e…
jvi.asm.org/content/95/6/e…
What does this mean in simple terms? Well, you raise T cells after natural infection or vaccines against 57 pieces of the spike protein and receptor binding domain of the virus. As authors write: "levels of SARS-CoV-2 neutralization antibodies alone do not determine protection"
And our vaccine trials SHOW us definitively that SARS-CoV-2 specific T cells are generated by the vaccines. The AZ vaccine "caused expansion of CD4+ and CD8+ T lymphocytes to specific epitopes of the spike protein. Of 87 spike-specific antigens identified"
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
by the sequencing, 75 remained unaffected by the B.1.351 mutations". So, T-cell responses should be generally unaffected by these variants. Excellent Dr. Jay Levy talked to me about this (HIV researcher from beginning ); said it reminded him a bit of all the talk and fear of
HIV superinfection at the beginning (that you could get another strain of HIV on top of yours & it would make HIV worse). Actually was quite rare and we could treat. So, let's just vaccinate, see what happens (like in Israel with B117, great response), not prophylactically worry
This is an amazing article about T cells that mirrors finding from other studies (see next tweet). Study looked at CD4+ and CD8+ T-cell memory in recovered COVID-19 patients (90) and close contacts (69). Size/ quality of memory T-cell pool of patients
nature.com/articles/s4146…
nature.com/articles/s4146…
better han those of close contacts. But still get strong proliferation capacity, size and quality of T-cell responses in close contacts; they are able to get immunity against SARS-CoV-2 even when lacking a detectable infection. Asymptomatic & symptomatic COVID-19 patients
exhibit similar levels of SARS-CoV-2-specific T-cell memory. This adds to many papers on this same phenomenon - even asymptomatic infection yields good T cell immunity. That & vaccines will get us there quickly (& depending on state and how much immunity they had before)
Two papers today about T cell responses to #covid19 being preserved against variants which can help lead to variant calming. First in OFID. Remember we have discussed before that coronaviruses have a high proofreading capability, mutate at low rates.
academic.oup.com/ofid/advance-a…
academic.oup.com/ofid/advance-a…
This study took 30 patients recovered from #covid19 to look at response of T cells against 3 variants of concern: B117 (UK), B.1.351 (S. Africa), P.1 (Brazil). All possess N501Y mutation in the receptor-binding domain (RBD) of the spike protein, target for neutralizing antibodies
If our T cell response against variants of concern are preserved, you will be protected against severe disease. And your T cell response is so complex! Prior study shows 132 SARS-CoV-2-specific CD8+ T cell responses corresponding to 52 unique epitopes
jci.org/articles/view/…
jci.org/articles/view/…
Means you form T cells against multiple parts of the virus & multiple parts of the spike protein. This new analysis showed only one mutation from B117, B.1.351, and P.1 overlapped with those 52 CD8+ T cell epitopes. So T cells from vax or infection will protect you from variants.
This paper is summarized nicely by an NIAID press release found here. "T cell response in convalescent individuals, and most likely in vaccinees, ...should offer protection against emerging variants."
nih.gov/news-events/ne…
nih.gov/news-events/ne…
So if vaccines (all) protect you against severe illness & T cell responses (likely responsible for that protection) preserved across variants - and the CDC found yesterday that vaccines protect us against infection as well as disease- vax is solution
cdc.gov/mmwr/volumes/7…
cdc.gov/mmwr/volumes/7…
One more EXCELLENT T-cell paper to add there. Performed serologic & T cell analysis (harder to do so not done that often) in 20 healthcare workers after 1st dose of Pfizer at days 7, 10, 21d after dosing. CD4 & CD8 cells seen as early as 7 days. cell.com/med/fulltext/S…
Peak CD8 activity by 21 days; peak CD4 by 10. Even before antibodies high. This is KEY point given that antibodies help stimulate cell-mediated immunity; latter usually inferred but in ALL of these vaccine studies, T cells measured directly so KNOW cell-mediated immunity develops

So mRNA vaccination induced early and functionally
efficient SARS-CoV-2 S-specific T cells (same level you get with asymptomatic infection) around time you get vaccine efficacy. Wondering if we should use all these detailed immunologic work to reframe reflexive immune thinking.
efficient SARS-CoV-2 S-specific T cells (same level you get with asymptomatic infection) around time you get vaccine efficacy. Wondering if we should use all these detailed immunologic work to reframe reflexive immune thinking.
Another paper on how CD4 (T cells) induced by COVID vax will cover variants. Here, authors spent some time showing mRNA vaccines for COVID will also protect you against common cold coronavirus but main question is: "Can variants escape T cell responses?"
jci.org/articles/view/…
jci.org/articles/view/…
"That is the critical question given the key role cellular immunity plays in controlling viral replication". So, gave Pfizer vax & looked whether generated T cells would
still recognize B.1.1.7 and B.1351 variants; CD4 cells generated against 23 epitopes (little pieces) of spike
still recognize B.1.1.7 and B.1351 variants; CD4 cells generated against 23 epitopes (little pieces) of spike
protein so few mutations across spike protein in these variants could not perturb that in-breadth response by the CD4 cells. Also confirmed this with CD4 response generated by Moderna vaccine. So, T cell response (which protects against severe disease) works well against variants

Wanted to add another paper to T cell thread looking at CD4 and CD8 responses after natural infection. 97% developed strong CD4 responses, despite variable symptoms. Despite waning antibody responses, the CD4 response remained strong out to 12 months
clinicalmicrobiologyandinfection.com/article/S1198-…
clinicalmicrobiologyandinfection.com/article/S1198-…
Importantly, CD4 more important than CD8 for SARS-CoV-2 protection. Discussion: "widely known that humoral immune response to coronaviruses variable & commonly short-lived while coronavirus-specific T-cell response more sustained and long-term detectable": pubmed.ncbi.nlm.nih.gov/2170159/
The long T cell immunity to SARS & MERS (severe coronaviruses) summarized in thread above. But even with mild coronaviruses, another paper showing us the durable T cell immunity response here. A nightly ode to the T cell
pubmed.ncbi.nlm.nih.gov/20554810/
pubmed.ncbi.nlm.nih.gov/20554810/
Good summary of the T cell response and how not to be concerned regarding variants by science reporter Julia Ries @namesjules on HealthLine:
healthline.com/health-news/co…
healthline.com/health-news/co…
Nothing like better than to reassure you how long T cell immunity after vaccination or natural infection is likely to last to 1) let you know why I don't think boosters will be necessary; 2) explain why protection from severe disease so high. This time from @UCSF own institution!
21 people had mild COVID-19 and Dr. Roan lab looked specifically at CD8 cell response (T cells: CD4 & CD8)- of note remember 1st SARS pandemic was 2002-2003 & CD8 cells still present (will be protective) 17 years later! Protect against acute infection but
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
also reservoir of long-lived memory cells if see infection again. Researchers tracked changes in CD8 cell response & able to determine, by their evolution and differentiation over 6 months that long-lived memory T cells will be produced (like SARS, 17 yrs, counting)
Can't find my thread on natural immunity so I will put this paper here with T cells. This is an important paper because (just like Dan J. Science 2020), looks at a broad range of immune responses (T cell, B cell, antibodies) with severe, mod, mild COVID
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
264 participants recruited from Atlanta and Seattle with mild, moderate, severe disease to look at convalescent immune responses. Most patients mount durable antibody, B and T cells specific for SARS-CoV-2 up to 250 days. Moreover, able to look at kinetics (half-lives) and clear
that these responses likely to achieve long-lived immunity after natural infection. Even after mild infection (71% of participants had mild disease; 24% moderate; 5% severe disease) although higher levels after severe. Half-lives of Ab, T cells show tell long-lived immunity.
Wow, this is truly best T cell paper I've seen where @SetteLab and colleagues show how complex your T cell response is after natural infection (will be true against spike protein in context of vaccines). First must define EPITOPE, which is a small piece
cell.com/cell-host-micr…
cell.com/cell-host-micr…
of the virus (protein) to which a single T cell can respond. We had already seen data in the thread above that T cells can respond to 82 or 52 epitopes across spike protein (which is what the vaccines have you raise an immune response against); this well done review in Cell
looked at 25 studies where T cell responses in natural infection measured to examine number of epitopes across the virus where they attack. Technical but there are different ways to measure T cells & commercial assays (coming on line) may not use fancy machines that give you more
granular information (e.g. ELISspot not granular). Across these 25 studies, @SetteLab identified 1400 unique epitopes (382 for CD4 and 1052 for CD8) across the virus where T cells respond (can attack). Epitopes from spike protein overrepresented, because more frequently studied.
In typically understated academic style, authors conclude "with more than 1400 epitopes , identified... unlikely that the new variants will escape T cell recognition, at either the population or individual level". T cells mature into memory & "go in bank"
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
• • •
Missing some Tweet in this thread? You can try to
force a refresh




