Images of Infectious Diseases
H&E of brain biopsy specimen.
Who is the host? What is the most likely pathogen? How do you treat?
#MayoIDQ
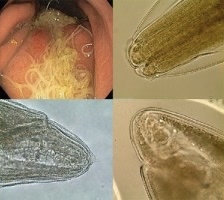
H&E of brain biopsy specimen.
Who is the host? What is the most likely pathogen? How do you treat?
#MayoIDQ

2/ #MayoIDQ
75F. Immunocompetent.
CC: headache x few months —> now left leg weakness, blurred vision, seizure. CBC/CMP normal. CT head: mass in right ventricle, pons. CT chest/abdomen for CA work up (-). Brain biopsy (photo).
Which of the following is the most likely pathogen?
75F. Immunocompetent.
CC: headache x few months —> now left leg weakness, blurred vision, seizure. CBC/CMP normal. CT head: mass in right ventricle, pons. CT chest/abdomen for CA work up (-). Brain biopsy (photo).
Which of the following is the most likely pathogen?
3/
Case diagnosis: cerebral #phaeohyphomycosis due to #cladophialophora
Note pigmented hyphae —> excludes Aspergillus (hyaline septate mould)
Among 3 remaining choices, the most common neurotrophic dematiaceous mould is Cladophialophora bantiana
Case diagnosis: cerebral #phaeohyphomycosis due to #cladophialophora
Note pigmented hyphae —> excludes Aspergillus (hyaline septate mould)
Among 3 remaining choices, the most common neurotrophic dematiaceous mould is Cladophialophora bantiana
4/
#Dematiaceous fungi - pigmented (melanin) septate hyphae
Alternaria
Bipolaris
Cladophialophora
Curvularia
Dactylaria
Exophiala
Phialophora
Verruconis
Wangiella
#Dematiaceous fungi - pigmented (melanin) septate hyphae
Alternaria
Bipolaris
Cladophialophora
Curvularia
Dactylaria
Exophiala
Phialophora
Verruconis
Wangiella
5/
Diseases caused by #dematiaceous fungi
#Chromoblastomycosis (note: copper penny bodies): Fonsecaea, Phialophora
#Eumycetoma (note: granular pus and sinus tracts): Madurella
#Phaeohyphomycosis (see next): multiple fungal agents
Diseases caused by #dematiaceous fungi
#Chromoblastomycosis (note: copper penny bodies): Fonsecaea, Phialophora
#Eumycetoma (note: granular pus and sinus tracts): Madurella
#Phaeohyphomycosis (see next): multiple fungal agents
6/
#Phaeohyphomycosis
1. Various pigmented fungi
2. Superficial local (onychomycosis, tinea)
3. Deep local (subQ, keratitis)
4. Tissue invasive: lung, CNS, osteomyelitis, peritonitis
5. Disseminated disease
#Phaeohyphomycosis
1. Various pigmented fungi
2. Superficial local (onychomycosis, tinea)
3. Deep local (subQ, keratitis)
4. Tissue invasive: lung, CNS, osteomyelitis, peritonitis
5. Disseminated disease
7/
CNS #Phaeohyphomycosis
1. Immunocompetent > ICH
2. Brain abscess/es
3. Headache and neuro s/s
4. Cladophialophora bantiana is most common cause >50%
5. Surgery + antifungals; high mortality
doi.org/10.1086/380635
CNS #Phaeohyphomycosis
1. Immunocompetent > ICH
2. Brain abscess/es
3. Headache and neuro s/s
4. Cladophialophora bantiana is most common cause >50%
5. Surgery + antifungals; high mortality
doi.org/10.1086/380635
• • •
Missing some Tweet in this thread? You can try to
force a refresh