Weekend Digest
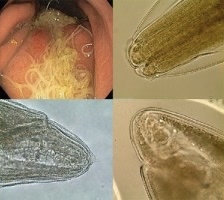
An Korean immigrant presented with early stage cholangiocarcinoma.
H & E stained tissue biopsy shown.
Name the pathogen and mechanism of infection.
An Korean immigrant presented with early stage cholangiocarcinoma.
H & E stained tissue biopsy shown.
Name the pathogen and mechanism of infection.

2/
Case Diagnosis:
#Clonorchis sinensis - oriental liver fluke
“The eggs of Clonorchis are practically indistinguishable from those of #Opisthorchis” (photo credit: CDC)
Case Diagnosis:
#Clonorchis sinensis - oriental liver fluke
“The eggs of Clonorchis are practically indistinguishable from those of #Opisthorchis” (photo credit: CDC)

3/
#Chlonorchis sinensis (and #Opistorchis)
Human infection is acquired by ingestion of undercooked, salted, pickled, or smoked freshwater fish (with metacercariae)
—> excyst in duodenum —> ascend biliary tree —> mature into adults in biliary ducts
cdc.gov/dpdx/clonorchi…
#Chlonorchis sinensis (and #Opistorchis)
Human infection is acquired by ingestion of undercooked, salted, pickled, or smoked freshwater fish (with metacercariae)
—> excyst in duodenum —> ascend biliary tree —> mature into adults in biliary ducts
cdc.gov/dpdx/clonorchi…

4/
#Chlonorchis sinensis (and #Opistorchis)
Clinical: inflammation / obstruction / mechanical injury of biliary ducts
Complications (cholangitis, cholelithiasis, cholecystitis, and cholangiocarcinoma), pancreatitis, and liver abscesses may develop.
ncbi.nlm.nih.gov/pmc/articles/P…
#Chlonorchis sinensis (and #Opistorchis)
Clinical: inflammation / obstruction / mechanical injury of biliary ducts
Complications (cholangitis, cholelithiasis, cholecystitis, and cholangiocarcinoma), pancreatitis, and liver abscesses may develop.
ncbi.nlm.nih.gov/pmc/articles/P…
5/
#Chlonorchis sinensis Rx
Praziquantel is treatment of choice
Alternative: albendazole
Plus: surgery if biliary obstruction and cancer
#Chlonorchis sinensis Rx
Praziquantel is treatment of choice
Alternative: albendazole
Plus: surgery if biliary obstruction and cancer
6/ Bonus tweet:
Name the liver fluke that is endemic in North America.
Name the liver fluke that is endemic in North America.
7/
#Metorchis conjunctus
Here is a report of common-source outbreak of 19 people who ate sashimi made from white sucker fish caught in a river in Montreal
Clinical: abdominal pain, eosinophilia, elevated liver enzymes + opistorchid eggs in stool
thelancet.com/pdfs/journals/…
#Metorchis conjunctus
Here is a report of common-source outbreak of 19 people who ate sashimi made from white sucker fish caught in a river in Montreal
Clinical: abdominal pain, eosinophilia, elevated liver enzymes + opistorchid eggs in stool
thelancet.com/pdfs/journals/…
• • •
Missing some Tweet in this thread? You can try to
force a refresh