
Over the past 10 months, we've tried to determine how COVID-19 affected some of the people most vulnerable to the virus: residents of long-term-care facilities.
covidtracking.com/analysis-updat…
covidtracking.com/analysis-updat…
Based on official state figures compiled by our team, as of March 4, 2021, at least 174,474 people had died of COVID-19 in long-term-care facilities. This represents 34% of the total deaths due to COVID-19 in the US. covidtracking.com/ltc-topline-es…
We estimate that as of March 2021, about 8 percent of people who live in US long-term-care facilities have died of COVID-19: Nearly one in 12. covidtracking.com/analysis-updat…
Because of data and reporting issues, these figures are known undercounts. The true toll of the pandemic among workers and residents in long-term-care facilities is higher than these figures can show.
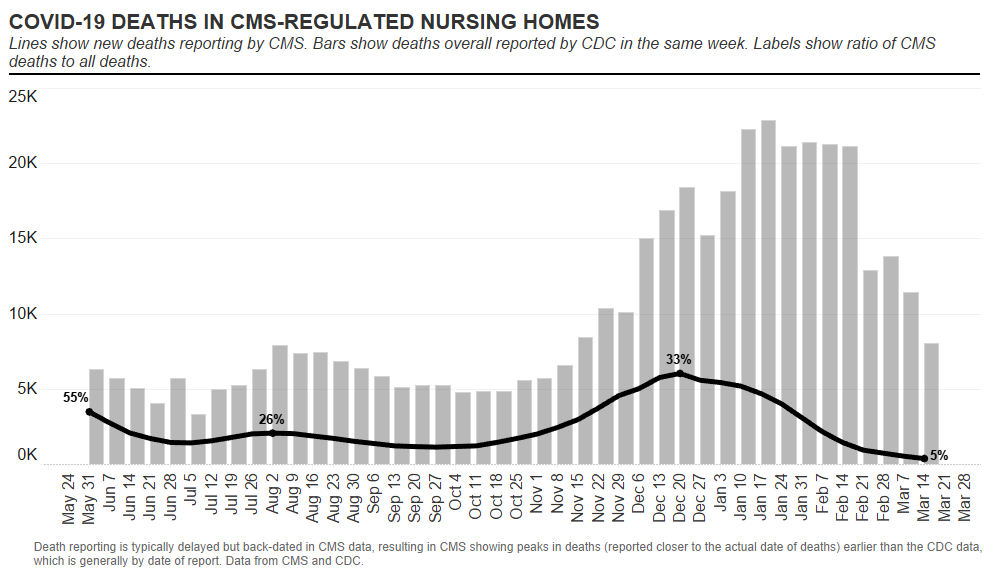
Some good news: The vaccines are working. All COVID-19 deaths have been declining for many weeks, but the share of these deaths that are associated with nursing-home outbreaks has declined substantially. 
To begin to protect our most vulnerable, regulators must change their approach to the oversight of these facilities—and this oversight must include mandatory data collection, rigorous analysis, and then swift action based on what the data reveals. covidtracking.com/analysis-updat…
• • •
Missing some Tweet in this thread? You can try to
force a refresh





