Prof Darrel Francis ☺ Mk CardioFellows Great Again
4 Apr,
36 tweets, 7 min read
When this happens ... 

What be your response?
Happily the plumber fixes it. He explains that this is a problem with blockage in the pipes that he had to clear.
You tell your neighbour about your lucky escape with your life.
You tell your neighbour about your lucky escape with your life.
A few months later, your neighbour starts to notice his sink being slow to drain. He realises that this too is caused by clogging up of the pipes, although not a catastrophic complete blockage.
What should he do?
What should he do?
First few answers are 100% correct.
Same problem, but less drastic version.
Same solution, but less urgent.
Same problem, but less drastic version.
Same solution, but less urgent.
When you have chest pain at rest, we have now trained the world to call 911 to get a stent put in to clear the blockage.
That is completely correct.
That is completely correct.
Since the right treatment of acute coronary syndrome is
"urgently go to hospital to get a stent",
then any sensible person (general physician or patient) will, default to assuming the right treatment of chronic stable angina is
"non-urgently go to hospital to get a stent".
"urgently go to hospital to get a stent",
then any sensible person (general physician or patient) will, default to assuming the right treatment of chronic stable angina is
"non-urgently go to hospital to get a stent".
Who is responsible for pointing out that this is not the case?
To put it in the words of Alex Nowbar and Chris Rajkumar (rcpjournals.org/content/clinme…)

You can't blame us for thinking that "ischemia kills". There is lots of observational evidence for it.
e.g. from CASS registry: Mortality versus number of diseased vessels
e.g. from CASS registry: Mortality versus number of diseased vessels

Many people have found it difficult to understand how the above graph can be true, and yet resolving ischaemia not dramatically slash mortality.
Here is the Nowbar-Rajkumar explanation.
Here is the Nowbar-Rajkumar explanation.

I no longer mock those who stumble on this trap of logic.
It is a VERY easy trap to fall into.
Here is a document whose origin I will not state, other than to say it was written and/or approved by over 100 named signatories.
One year after ISCHEMIA reported.
See highlight.
It is a VERY easy trap to fall into.
Here is a document whose origin I will not state, other than to say it was written and/or approved by over 100 named signatories.
One year after ISCHEMIA reported.
See highlight.

At a meeting I showed this slide and asked some of the authors:
(a) Is the y axis cumulative or instantaneous? And if it is cumulative, why does it have bumps that go up and then down?
(a) Is the y axis cumulative or instantaneous? And if it is cumulative, why does it have bumps that go up and then down?
(b) What revascularisation strategy halves the rate of CV events compared with chronic stable disease?
(c) Most poignantly, what form of revascularisation causes the NON-revascularised arm to have a step up in events at time zero?

Result?
They were very angry. This surprised me, because they presumably they hadn't been so angry when the signed the document.
Specifically:
(a) They refused to be pinned down on whether it is cumulative or instantaneous. "It's just to give the feeling." (!)
They were very angry. This surprised me, because they presumably they hadn't been so angry when the signed the document.
Specifically:
(a) They refused to be pinned down on whether it is cumulative or instantaneous. "It's just to give the feeling." (!)
(b) They refuse to suggest what form of procedural intervention halves the event rate chronically from day 1.
I offered the suggestion that perhaps the diagram shows a statin tablet, not a balloon?
Oddly this generously-offered escape route did not resolve their frowns.
I offered the suggestion that perhaps the diagram shows a statin tablet, not a balloon?
Oddly this generously-offered escape route did not resolve their frowns.
(c) "We don't have to have a reason for the vertical positioning at the beginning".
So Figure 1 of the paper is one where:
- they don't know what the Y axis is
- they don't feel responsible for the relative slopes
- they don't feel responsible for the vertical positioning
- they don't know what the Y axis is
- they don't feel responsible for the relative slopes
- they don't feel responsible for the vertical positioning
Some people are excited that thallium scanning predicts CV events.
But the same is true for exercise testing.
And Stress Echo
And Stress MRI
Let's face it, the same is true for asking patients their age, or just seeing if they look bald.
But the same is true for exercise testing.
And Stress Echo
And Stress MRI
Let's face it, the same is true for asking patients their age, or just seeing if they look bald.
Here are a few graphs. I can't be bothered telling you which one is which modality.

It's Exercise testing, stress echo and thallium
Or maybe
Exercise stress Echo,
Smoking status and
Baldness quotient
Exercise stress Echo,
Smoking status and
Baldness quotient
If you are really bored you can read the paper and work out which is which, but I wouldn't bother. It's not a good use of your time.
Francis's First Law of Prognostic Markers
"ANY FEATURE OF A DISEASE,
IS A PROGNOSTIC MARKER OF THAT DISEASE,
Obviously, Duh."
"ANY FEATURE OF A DISEASE,
IS A PROGNOSTIC MARKER OF THAT DISEASE,
Obviously, Duh."
So why would having INDUCIBLE ischaemia make you die?
I think all are plausible answers. It is entirely plausible that having episodes of ischaemia kill you.
Just like having episodes of asthma, even if they are not fatal, might gradually cause some sort of injury to the lung (inflammatory cells and whatnot), who knows? Plausible.
Just like having episodes of asthma, even if they are not fatal, might gradually cause some sort of injury to the lung (inflammatory cells and whatnot), who knows? Plausible.
And even the argument "If god had meant us to have ischaemia, he would have given us all ischaemia" carries weight with me.
I have difficulty believing it is beneficial to acquire inducible ischaemia (although I know some people argue the point with preconditioning etc).
I have difficulty believing it is beneficial to acquire inducible ischaemia (although I know some people argue the point with preconditioning etc).
In the Nowbar-Rajkumar thesis:
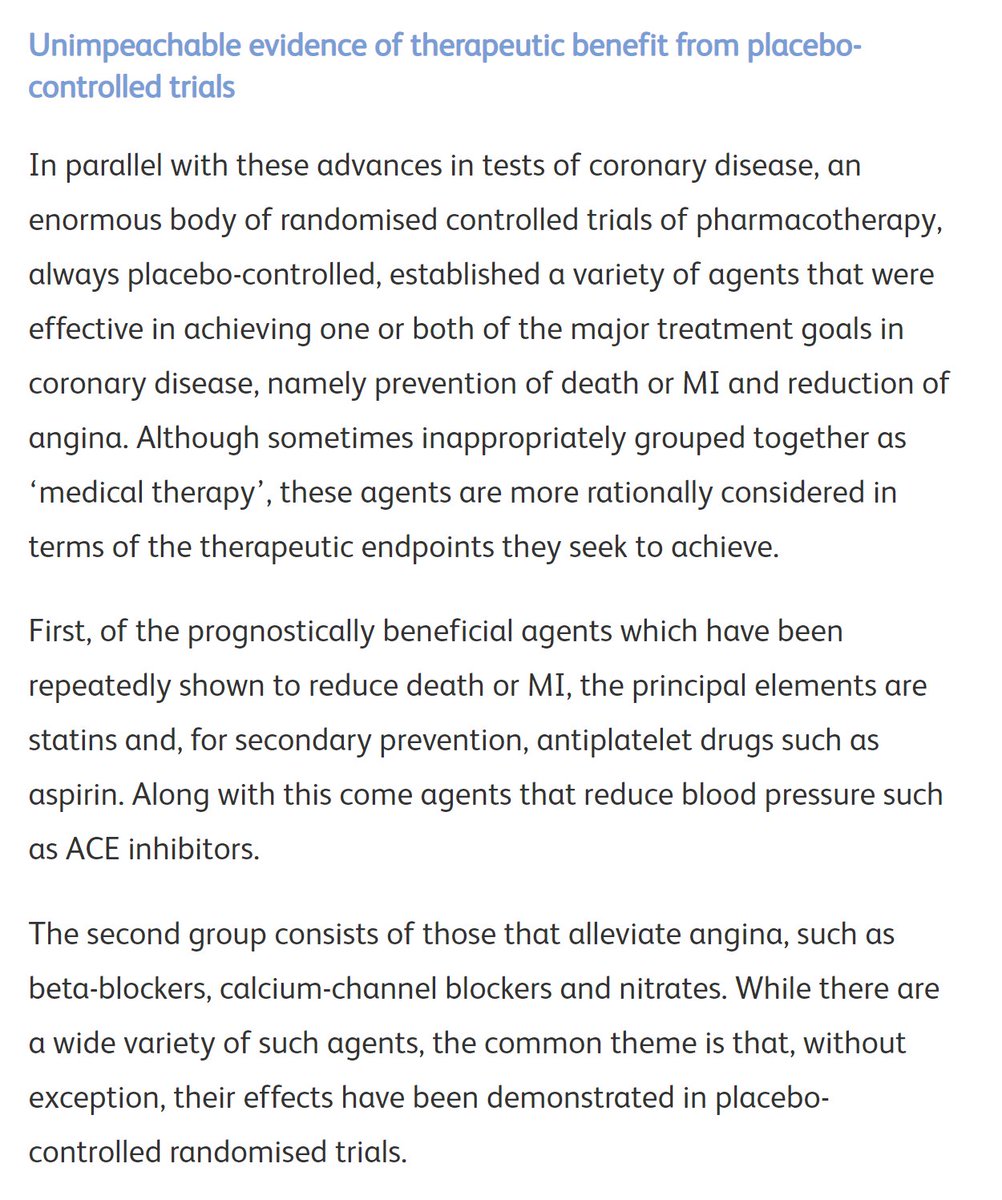
A summary of COURAGE and its biggest flaw:

With the confirmed safety in the COURAGE cohort, ISCHEMIA could take the very difficult next step to prevent that flaw.

COURAGE and ISCHEMIA revealed our glistening edifice to be less solid than we had assumed.
Time to retreat.
Time to retreat.
Time to retreat!
"Take the outer city, we don't care! It's just some rubbish buildings we never liked anyway."
"We never believed revascularisation would improve prognosis! (even though we still secretly do: just look at the green bar graphs! look at Mystery Figure 1!)"
"Take the outer city, we don't care! It's just some rubbish buildings we never liked anyway."
"We never believed revascularisation would improve prognosis! (even though we still secretly do: just look at the green bar graphs! look at Mystery Figure 1!)"
We can barricade ourselves into the inner sanctum of the citadel, for the last stand.
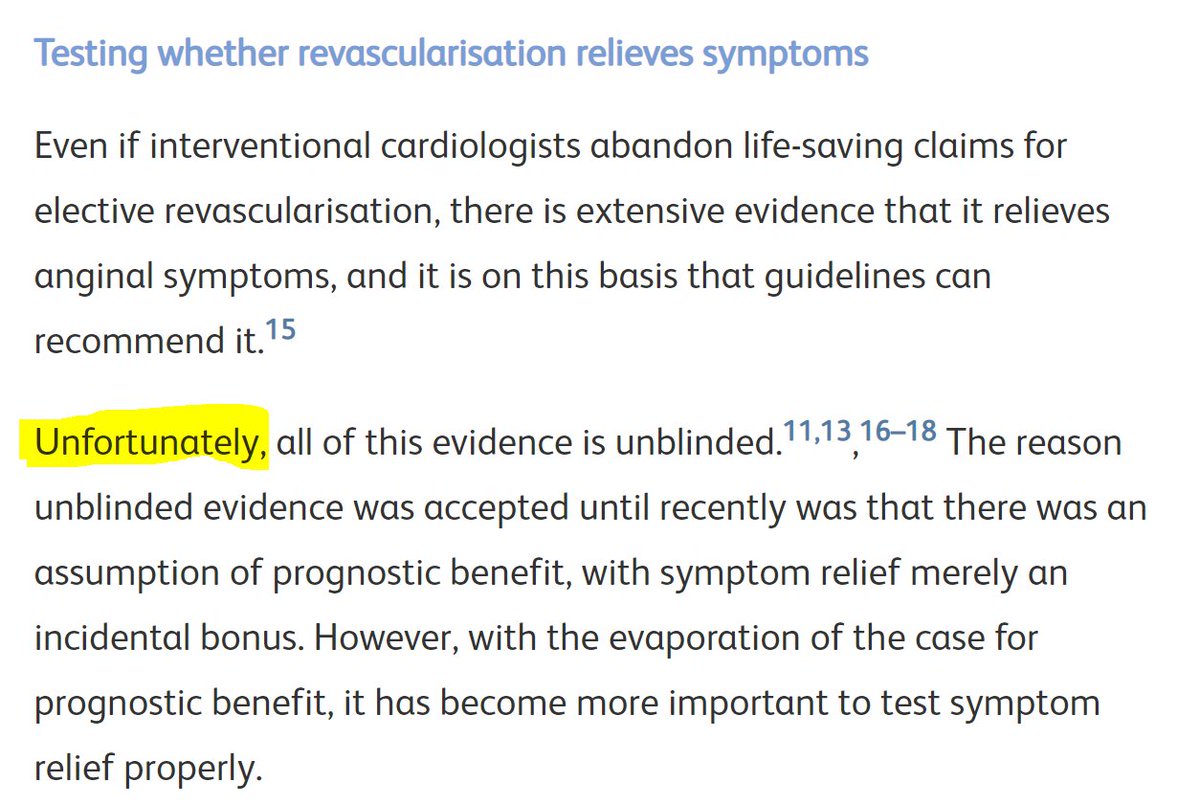
Symptoms.
"At least the damn things stops you getting angina!
We know that for 100% certain. Don't we?"
Symptoms.
"At least the damn things stops you getting angina!
We know that for 100% certain. Don't we?"
What happened next?
I won't spoil your fun.
Read the whole story here:
rcpjournals.org/content/clinme…
I won't spoil your fun.
Read the whole story here:
rcpjournals.org/content/clinme…
• • •
Missing some Tweet in this thread? You can try to
force a refresh