Prof Darrel Francis ☺ Mk CardioFellows Great Again
17 Apr,
23 tweets, 4 min read
I do admit I pour vitriol on fellows who say NYHA is 2 to 3.
8-)
"Whats the point of going to medical school and then training in cardiology? Could have just gone to the pub."
8-)
"Whats the point of going to medical school and then training in cardiology? Could have just gone to the pub."
https://twitter.com/doc_ccc/status/1382587943525695488
NYHA has 4 possible values.
The cleaner could tell the people in NYHA 1: they are basically feeling normal.
The cleaner could also tell people in NYHA 4. They are slumped in a chair or bed, breathless at rest.
Everyone else is in 2 or 3.
The cleaner could tell the people in NYHA 1: they are basically feeling normal.
The cleaner could also tell people in NYHA 4. They are slumped in a chair or bed, breathless at rest.
Everyone else is in 2 or 3.
Therefore the entire purpose of the 10 years of medical school, cardiology training, PhD and whatnot, is to be more skilled than the cleaner, i.e. to be able to distinguish NYHA 2 from 3.
What I don't tell the fellows is that although I am always confident in classifying patients as NYHA 2 versus 3, my performance in this task was tested by Claire Raphael...
google.com/url?sa=t&sourc…
google.com/url?sa=t&sourc…
In short, I am excellent at classifying patients into 2 versus 3.
In my own opinion.
It's only when you compare to other people's opinion that you realise I might be talking rubbish.
In my own opinion.
It's only when you compare to other people's opinion that you realise I might be talking rubbish.
The solution that I have evolved is to never ask anyone else's opinion (other than people who work for me and so have to agree with me).
Ignorance is bliss.
Ignorance is bliss.
Heh heh, I wouldn't be so harsh as David (for once in my life!)
https://twitter.com/djc795/status/1383235697218256899?s=19
The strange thing is, NYHA is extremely prognostic.
If I recall correctly, it is more prognostic than EF, by even the most sophisticated methods.
If I recall correctly, it is more prognostic than EF, by even the most sophisticated methods.
So when you want to asses prognosis in a patient, you have a choice.
Buy a million dollar MRI scanner to calculate EF.
Or just wink at the janitor and ask him to come over and speak to the patient.
The Janitor will win, and you will save yourself the million.
Buy a million dollar MRI scanner to calculate EF.
Or just wink at the janitor and ask him to come over and speak to the patient.
The Janitor will win, and you will save yourself the million.
That's how important symptoms are.
Even if they are hard to measure.
Even if we are not very good at selecting scales (thanks Todd Lee for pointing out the Duke Scale, and of course there are proprietary pay-to-ask scales like Minnesota)
Even if they are hard to measure.
Even if we are not very good at selecting scales (thanks Todd Lee for pointing out the Duke Scale, and of course there are proprietary pay-to-ask scales like Minnesota)
Even if we are unclear on how to use the scales (as the Raphael study above shows is the case for NYHA).
*Still* symptoms trump the fanciest, most expensive tests we can do.
That's why I do like symptoms.
*Still* symptoms trump the fanciest, most expensive tests we can do.
That's why I do like symptoms.
Even though we don't in reality know what to do about 2 versus 3, we get it generally right in the sense that the people I put into 3 do worse than those I put into 2.
Even though you would divide the patient's up differently, and your 3s would do worse than your 2s.
It's all OK, in a way, as long as we do not have even the slightest motivation to tilt the answer one way or the other.
Where it goes wrong, however, as David points out, is when we have a preference, which is in two situations.
1. When we are the gatekeeper to a study, and the patient "needs to be in NYHA 3" to get in. 

If any fellows are out there are bored they might enjoy looking at the control arms of trials which only took NYHA 3 (or the NYHA stratum of trials that took 3 and 4) and compare with observational cohorts of NYHA 3. I bet you the trials have been generous in what is 3.
Which is why I used to laugh at the requirement for people to have NYHA 3 to get spironolactone following RALES.
"Yes the poor guideline writers had to say that, but think about how people were recruiting for RALES. If you had someone who managed to have an EF under 35 and was happy to be in the trial, do you think you would be unbiased in making up their NYHA number?"
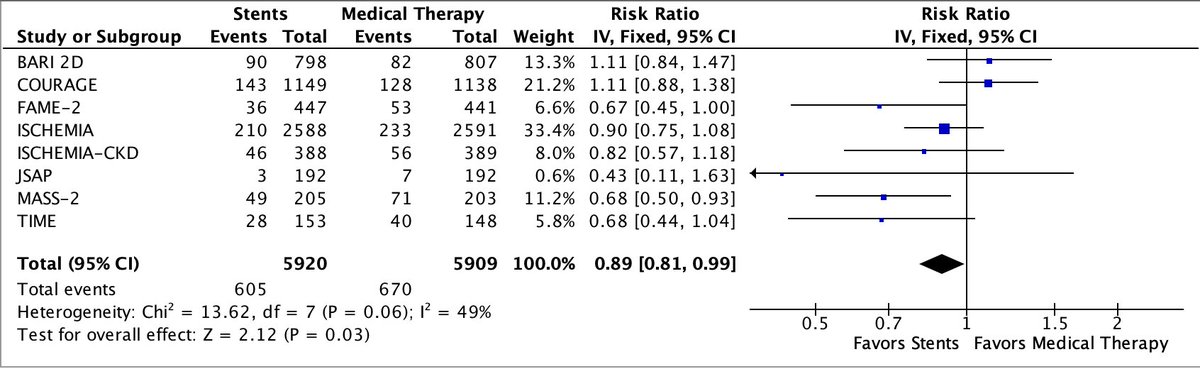
2. The other time we can't be trusted to be unbiased is when it is a trial endpoint AND we know which arm the patient is in.

Because, well.
I don't know how to put this.
Ummmm.
I don't know how to put this.
Ummmm.
Let me just show you the paradigm case of what happens, and leave you to comment.

• • •
Missing some Tweet in this thread? You can try to
force a refresh