Up next - Update on TMA! (thrombotic microangiopathy) at #ASPHO2021 Thread here 1/n
Transplant associated-TMA (TA-TMA) defined here. Look at the labs that you should use to help guide this diagnosis. High risk criteria of TA-TMA on second slide. 2/n 
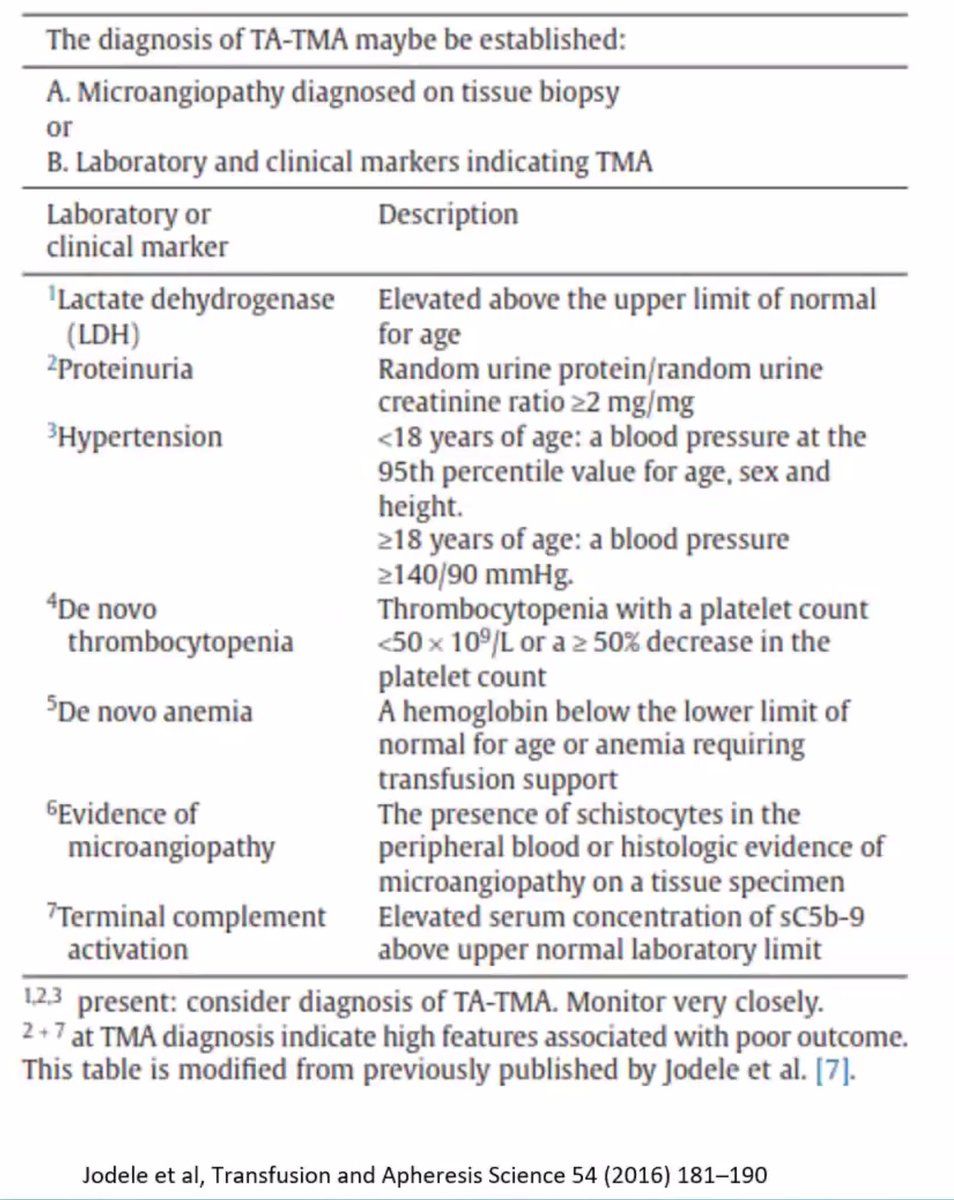

TA-TMA have a really high morbidity with a lot of multiorgan injury (intestinal, pulmonary, CNS)... scary -- I don't see this often (since I am no longer working in transplant patients) but the information can be translatable to other TMA type processes. 3/n

I need this reminder all the time as I continue to learn about this -- complement. Terminal complement activation is measured by elevations in cC5b-9. C5 blockage (eculizumab) is treatment for TA-TMA. With this 1 yr OS from 16.7 to 66% w/ this therapy. 4/n
When it's not working - think about high eculizumab clearance, high complement generation when there's a lot of inflamm (esp with GI-TMA) -- so think about personalized PK for these patients and know that you have to follow complement levels (CH50 and C5b9) to resolution. 5/n
Dr. Jodele's summary here for risk stratification and treatment for TA-TMA. Thanks for sharing at #ASPHO2021 - a good reminder for me about complement inhibition! 5/5


• • •
Missing some Tweet in this thread? You can try to
force a refresh