This outbreak is vital to understand. It shows what we still face if younger folks go unvaccinated.
47% of health care workers refused vax, while only 10% of residents did.
Result: 1 unvax'd HCW with COVID led to 20 HCWs & 26 residents infected, of whom 3 died (1 vaccinated).
47% of health care workers refused vax, while only 10% of residents did.
Result: 1 unvax'd HCW with COVID led to 20 HCWs & 26 residents infected, of whom 3 died (1 vaccinated).
https://twitter.com/nytimes/status/1384980269984370692
Let's unpack the details.
Q: Did the vax (2 doses of Pfizer) work? Absolutely. It was remarkable - but not perfect.
-Of 8 unvax residents, 6 got COVID (75% attack rate), 2 died (33% death rate).
-Of 71 vax residents, 18 got COVID (25%), 1 died (6%).
cdc.gov/mmwr/volumes/7…
Q: Did the vax (2 doses of Pfizer) work? Absolutely. It was remarkable - but not perfect.
-Of 8 unvax residents, 6 got COVID (75% attack rate), 2 died (33% death rate).
-Of 71 vax residents, 18 got COVID (25%), 1 died (6%).
cdc.gov/mmwr/volumes/7…
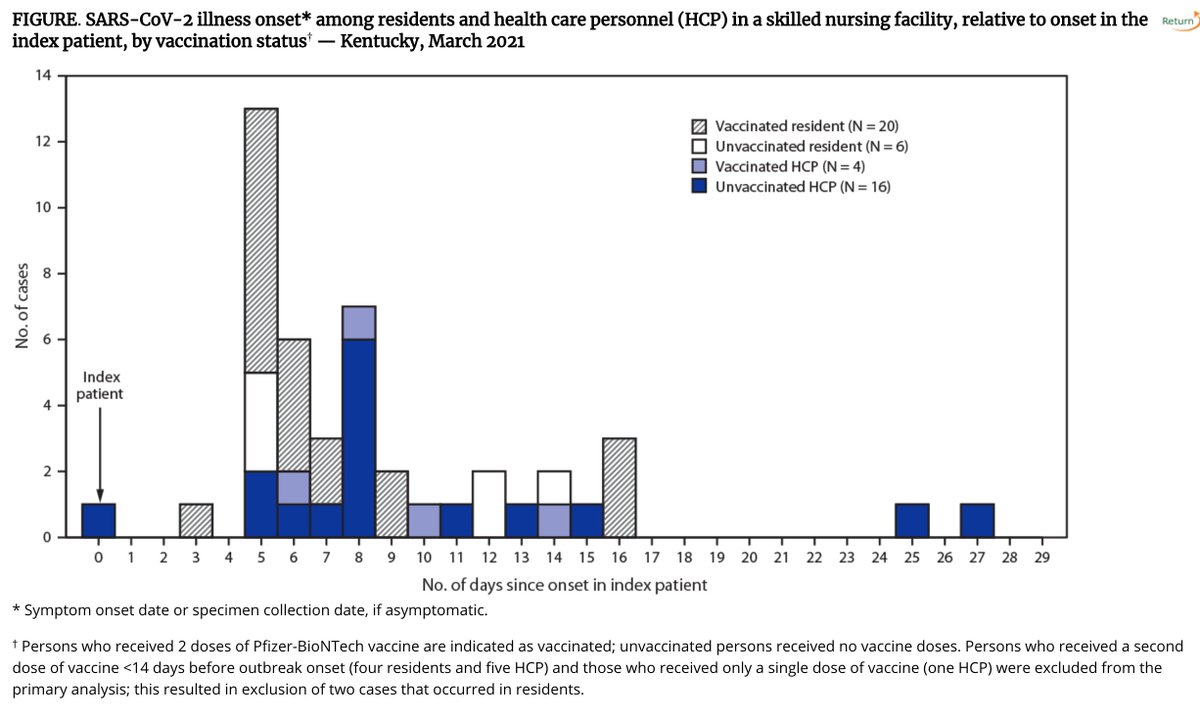
Vaccine effectiveness against symptomatic infection was 87%. Protection against death was 94%.
Clearly, in nursing homes, protection against death is not 100%. Why? Residents are more frail. The virus was also a new variant (R1) which might have had slightly reduced vax effect.
Clearly, in nursing homes, protection against death is not 100%. Why? Residents are more frail. The virus was also a new variant (R1) which might have had slightly reduced vax effect.
Also clear: a 50% vaccination rate for HCWs in such settings is not acceptable.
This case tells me that requiring COVID vaccination, just like flu vaccination, for working with vulnerable patients is going to be necessary.
This case tells me that requiring COVID vaccination, just like flu vaccination, for working with vulnerable patients is going to be necessary.
• • •
Missing some Tweet in this thread? You can try to
force a refresh