Genetic testing: there are so many tests to choose from! Karyotype, Microarray, Whole exome sequencing, they all sound the same. What's the difference? Read on and hopefully things will become clear... 🧵
#meded #tweetorial #medgen
#meded #tweetorial #medgen
First, let's remember that our DNA is found in really nice organized packages called chromosomes. Humans have 23 pair of chromosomes = 46 in total. Each chromosome has a short arm (p=petit) and a long arm (q=comes after p). 
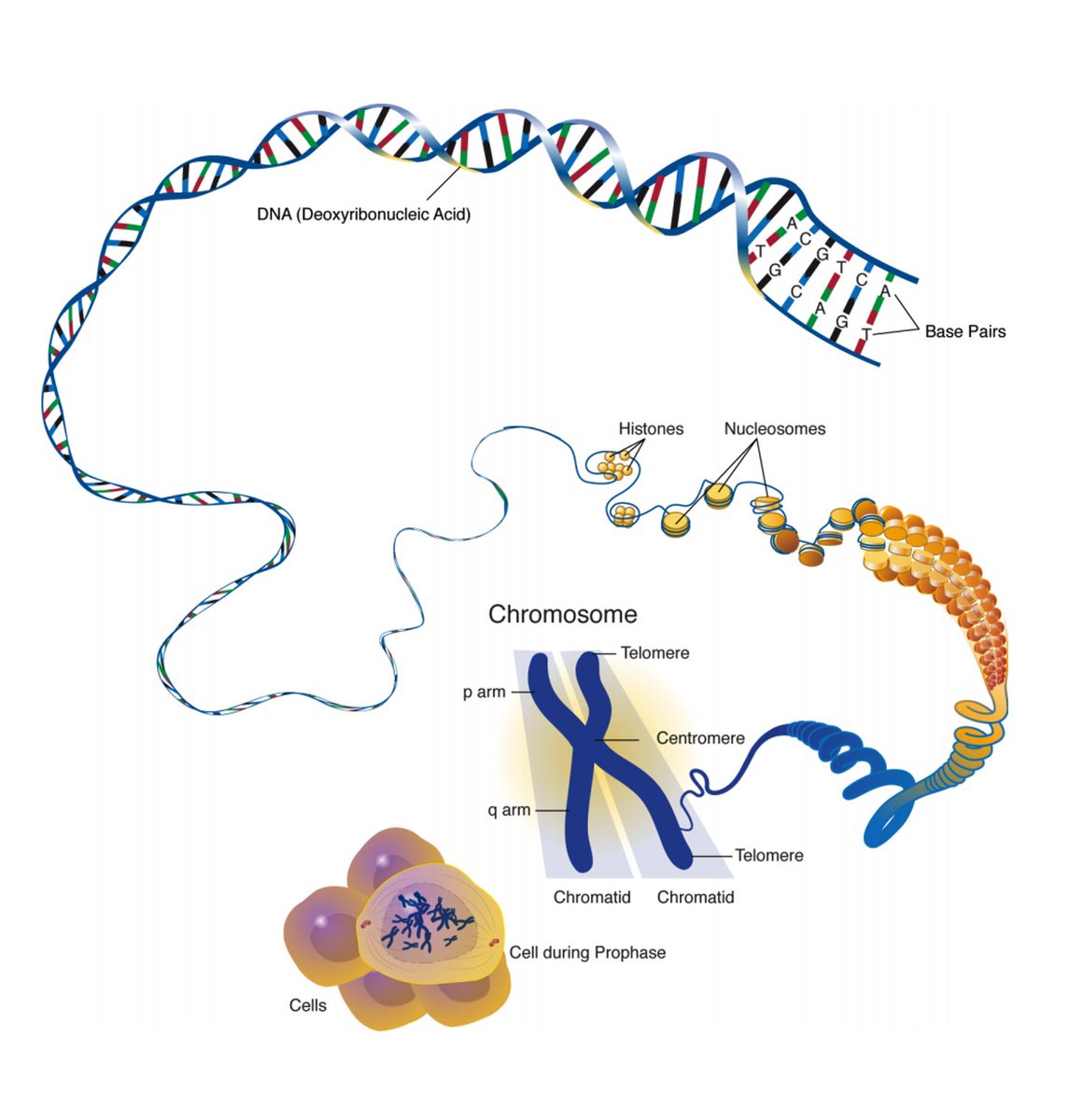
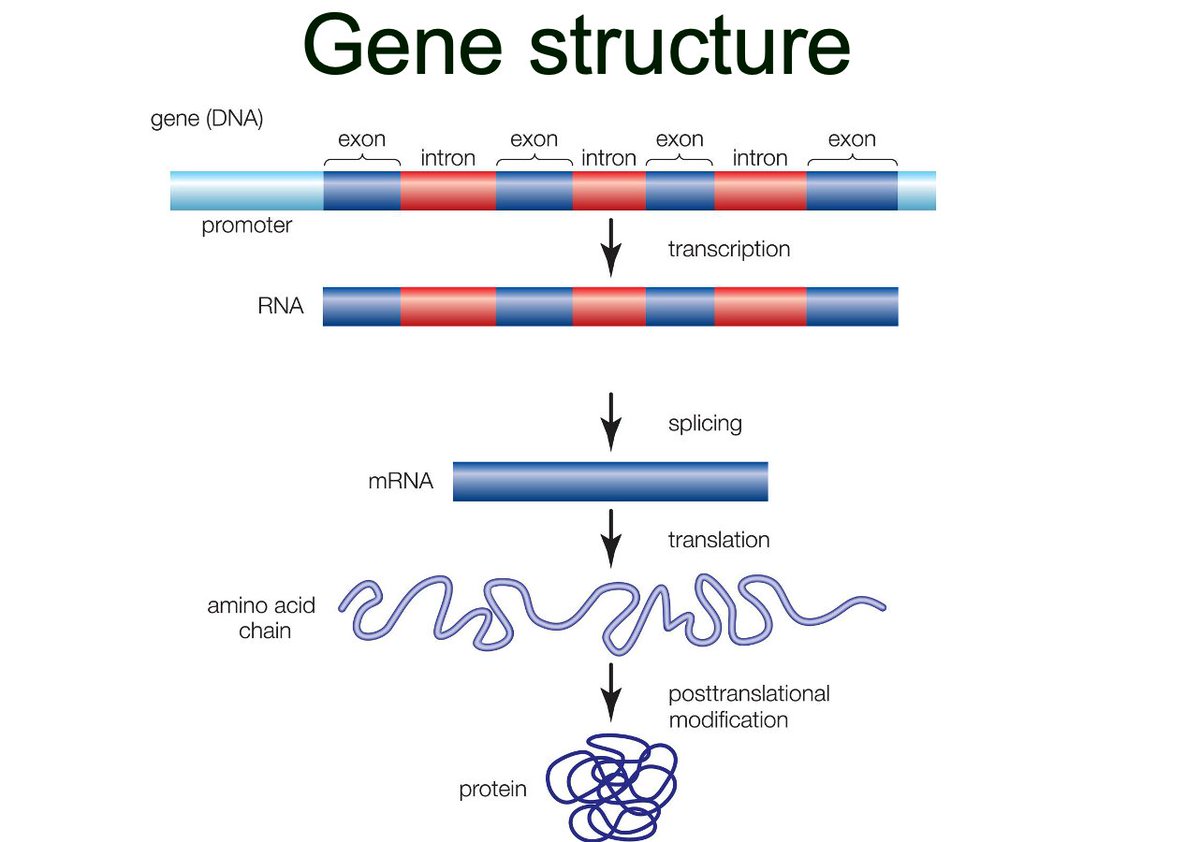
Genes are segments of DNA where each codes for a specific protein.
Genes are found along chromosomes in a predictable location and order. For example, the CFTR gene is found on the long arm of chromosome 7 in all humans.
Genes are found along chromosomes in a predictable location and order. For example, the CFTR gene is found on the long arm of chromosome 7 in all humans.


OKAY, I CANNOT STRESS THIS POINT ENOUGH. There are different tests to look at mutations in
1. Chromosomes (blue tests) vs.
2. Genes (orange tests).
See how the blue and orange tests don't really overlap? They are looking at different sized genetic changes.
1. Chromosomes (blue tests) vs.
2. Genes (orange tests).
See how the blue and orange tests don't really overlap? They are looking at different sized genetic changes.

The main chromosome tests are:
1. Karyotype
2. FISH
3. Microarray
Imma gonna teach you the differences
1. Karyotype
2. FISH
3. Microarray
Imma gonna teach you the differences

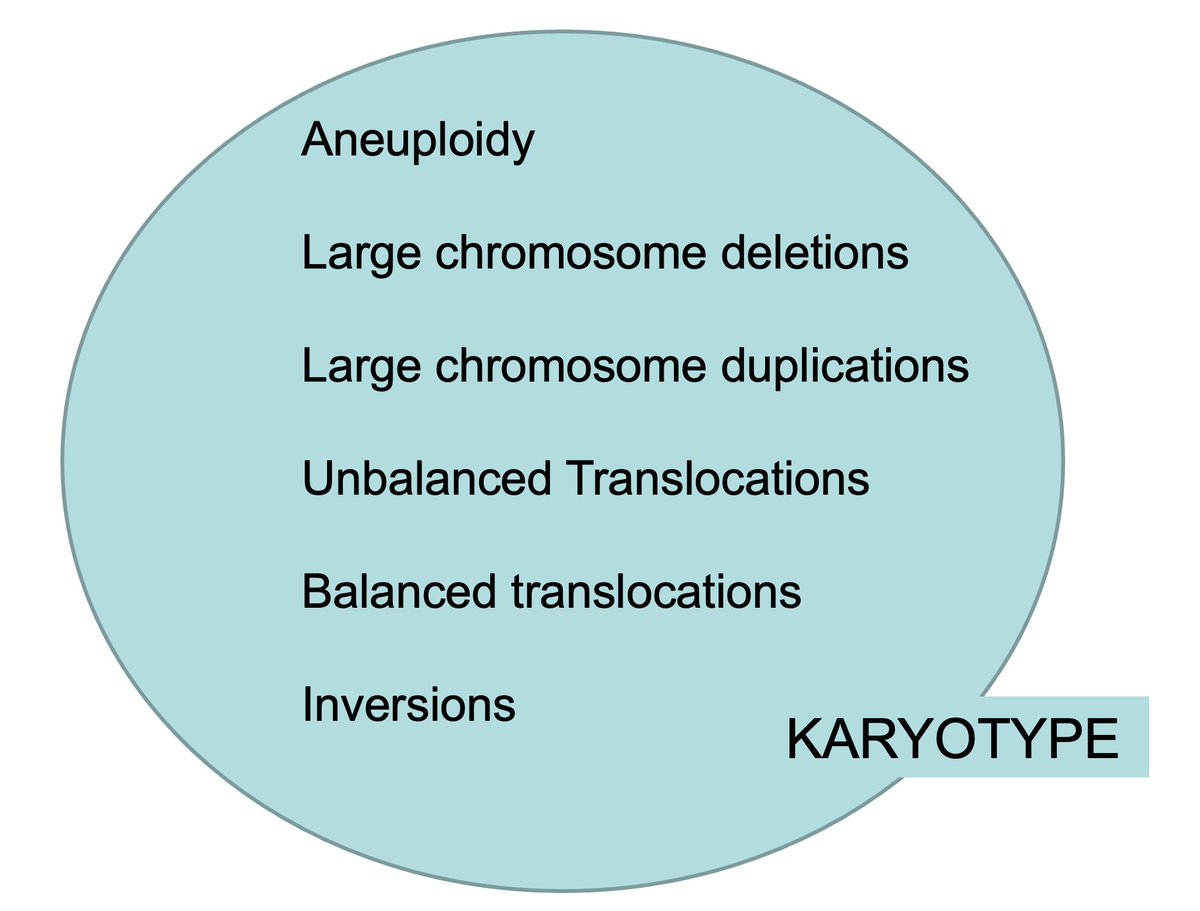
1. Karyotype
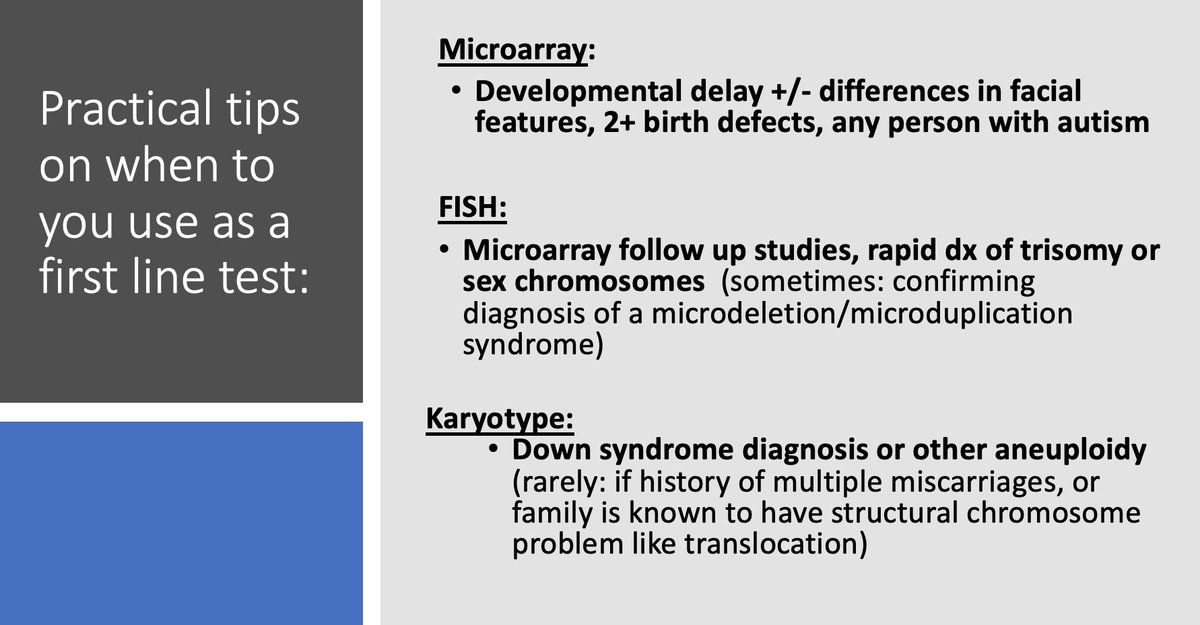
This is a really good test for looking at chromosome number, large changes to the chromosomes, and its structure. But it's not really good at looking at the chromosomes in fine detail. That's why we rarely use the test anymore. We have better tests now.
This is a really good test for looking at chromosome number, large changes to the chromosomes, and its structure. But it's not really good at looking at the chromosomes in fine detail. That's why we rarely use the test anymore. We have better tests now.

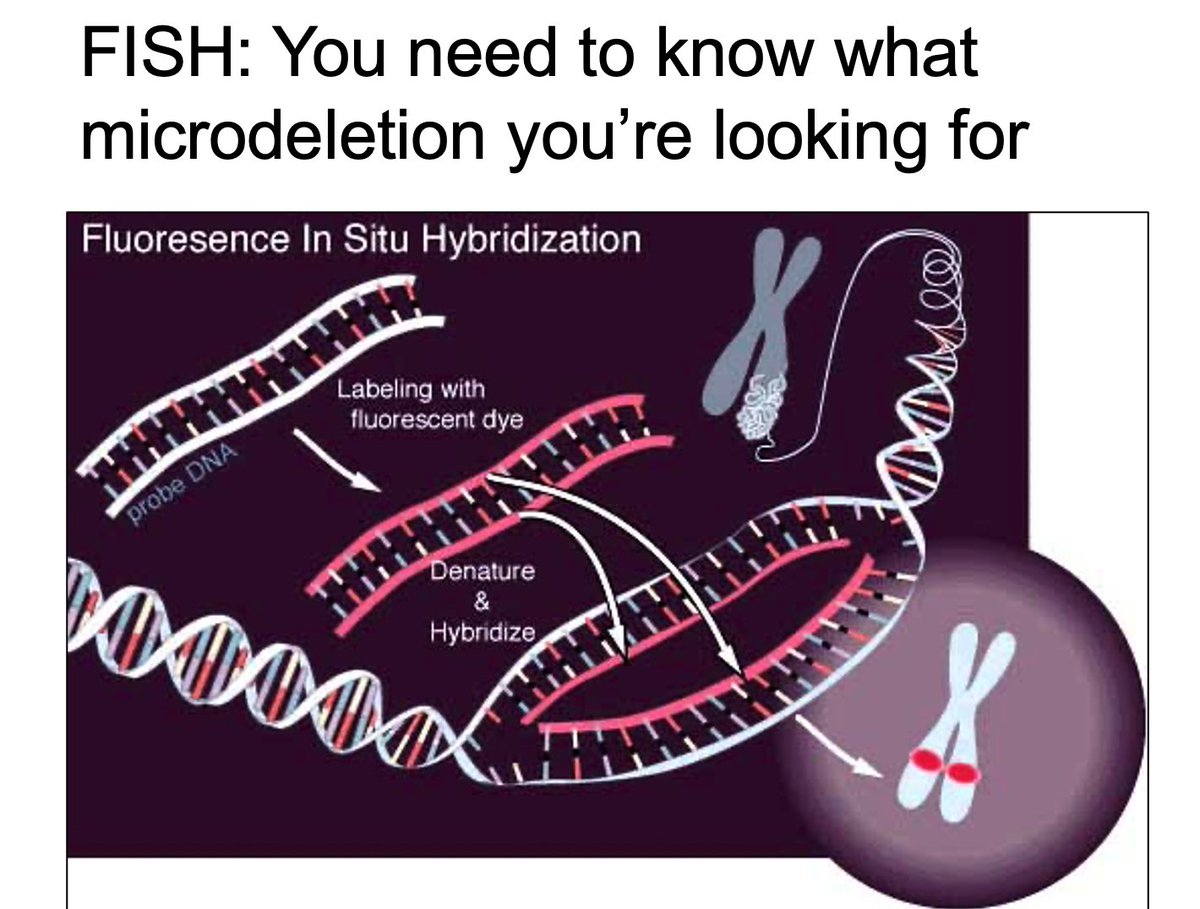
2. FISH (Fluorescence In Situ Hybridization)
There are chromosome deletions and dups that are too small to be seen on karyotype (microdeletion/microdup). That's when you can use FISH! But you need to know exactly the region you're interested in (eg. 22q.11 FISH for Digeorge).
There are chromosome deletions and dups that are too small to be seen on karyotype (microdeletion/microdup). That's when you can use FISH! But you need to know exactly the region you're interested in (eg. 22q.11 FISH for Digeorge).

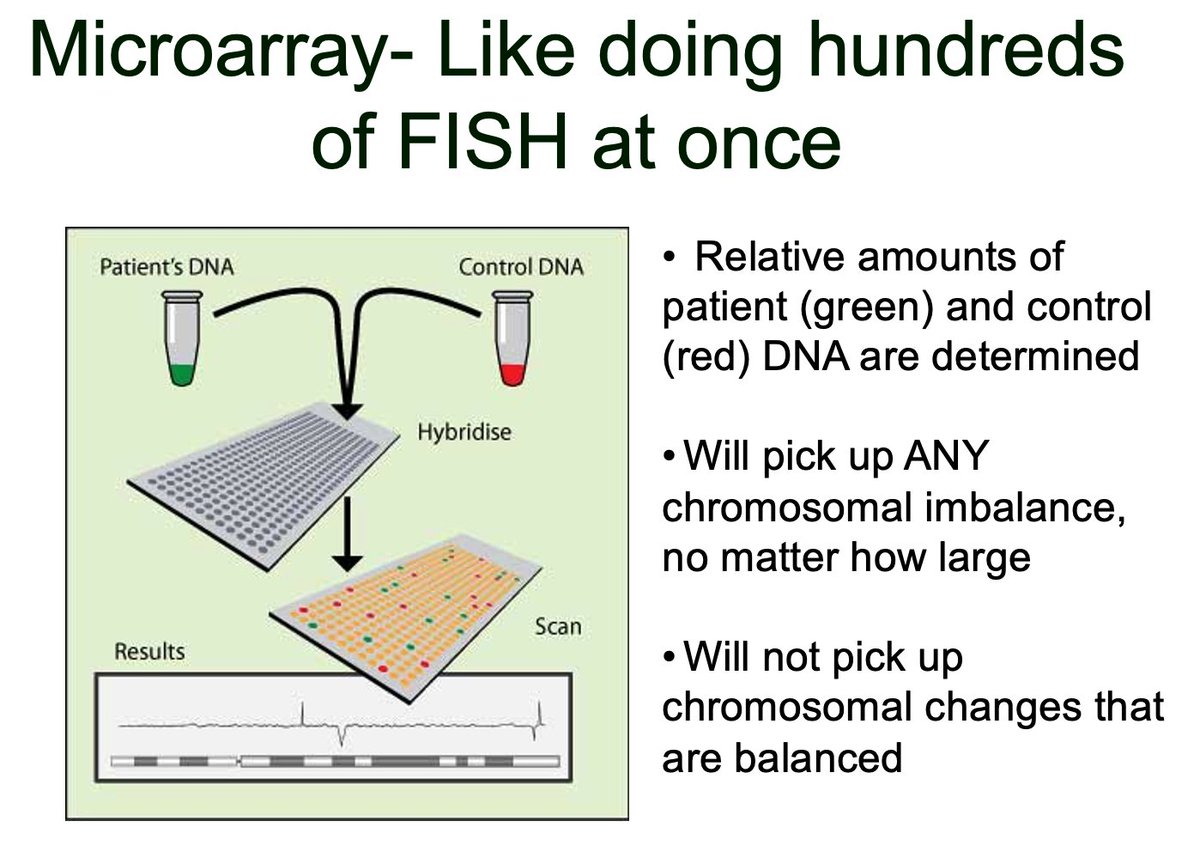
3. Microarray
This test will detect ANY size imbalance in chromosomes including microdel/dups, may miss balanced changes. Thankfully, most chromosome diseases are caused by imbalance. That's why microarray is the bomb diggity of chromosome tests.
This test will detect ANY size imbalance in chromosomes including microdel/dups, may miss balanced changes. Thankfully, most chromosome diseases are caused by imbalance. That's why microarray is the bomb diggity of chromosome tests.

IN summary: if you're suspecting a chromosomal disorder, send a MICROARRAY.
Rarely do you need a karyotype or FISH. If you are thinking of sending these, you may want to talk to a genetic counsellor, geneticist, or lab first. We good?
Rarely do you need a karyotype or FISH. If you are thinking of sending these, you may want to talk to a genetic counsellor, geneticist, or lab first. We good?
Okay, what about the other non-chromosome tests, the orange tests on that previous slide? AND WHEN AM I GOING TO TALK ABOUT AN EXOME?
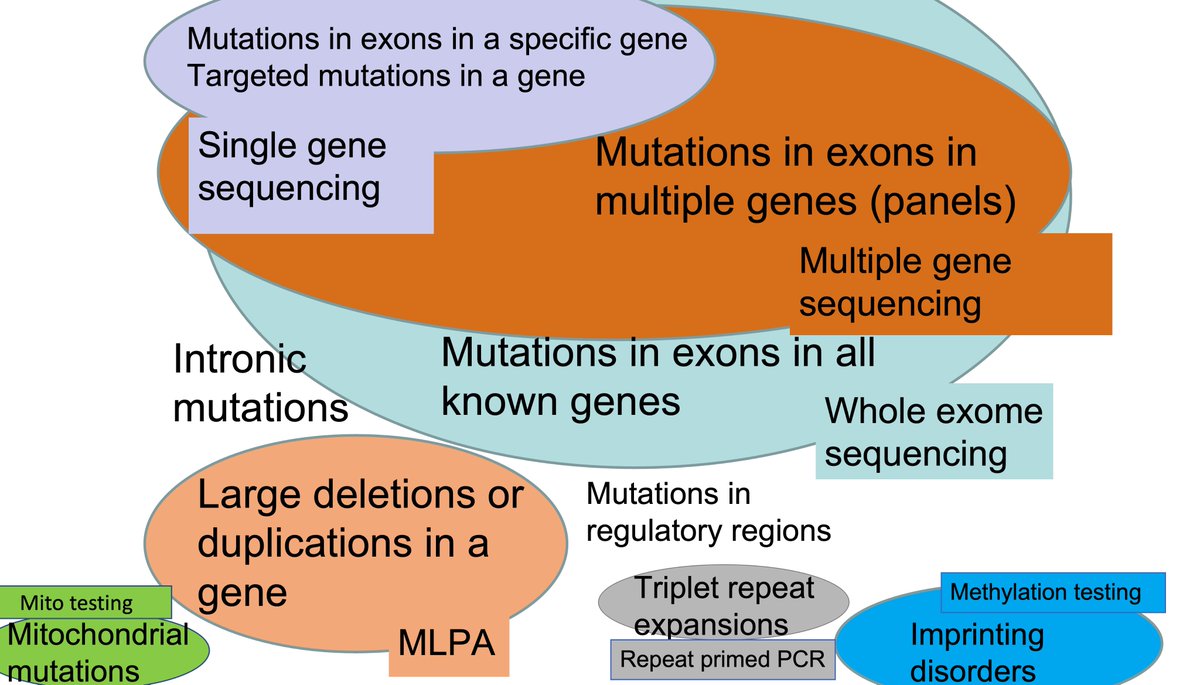
There are different tests that look at your GENES.
There are different tests that look at your GENES.
There are many gene-based tests:
A. Targeted sequencing
B. Whole exome sequencing
C. MLPA/deletion duplication testing
D. Repeat expansion testing
E. Methylation testing
F. Mitochondrial sequencing
A. Targeted sequencing
B. Whole exome sequencing
C. MLPA/deletion duplication testing
D. Repeat expansion testing
E. Methylation testing
F. Mitochondrial sequencing
Let's start with our favourite, SEQUENCING. Recall that genes contain exons that actually code for the protein. Sequencing is great at picking up common gene variants (SNVs and small Indels) and mainly within exons.

The main sequencing tests are:
A: Targeted sequencing of specific gene(s): Single gene testing (eg. CFTR) OR Multiple genes (eg. Epilepsy panel)
B: Whole exome sequencing: Sequence all exons of disease genes at once
It's not without its limitations, but it's a darn good test.
A: Targeted sequencing of specific gene(s): Single gene testing (eg. CFTR) OR Multiple genes (eg. Epilepsy panel)
B: Whole exome sequencing: Sequence all exons of disease genes at once
It's not without its limitations, but it's a darn good test.


C. MLPA (deletion/duplication testing)
What if there was a deletion or duplication within the DNA that was larger than a few nucleotides (like say several exons large), but MUCH smaller than a chromosome microdeletion/duplication? You can use a test called MLPA to pick these up.
What if there was a deletion or duplication within the DNA that was larger than a few nucleotides (like say several exons large), but MUCH smaller than a chromosome microdeletion/duplication? You can use a test called MLPA to pick these up.

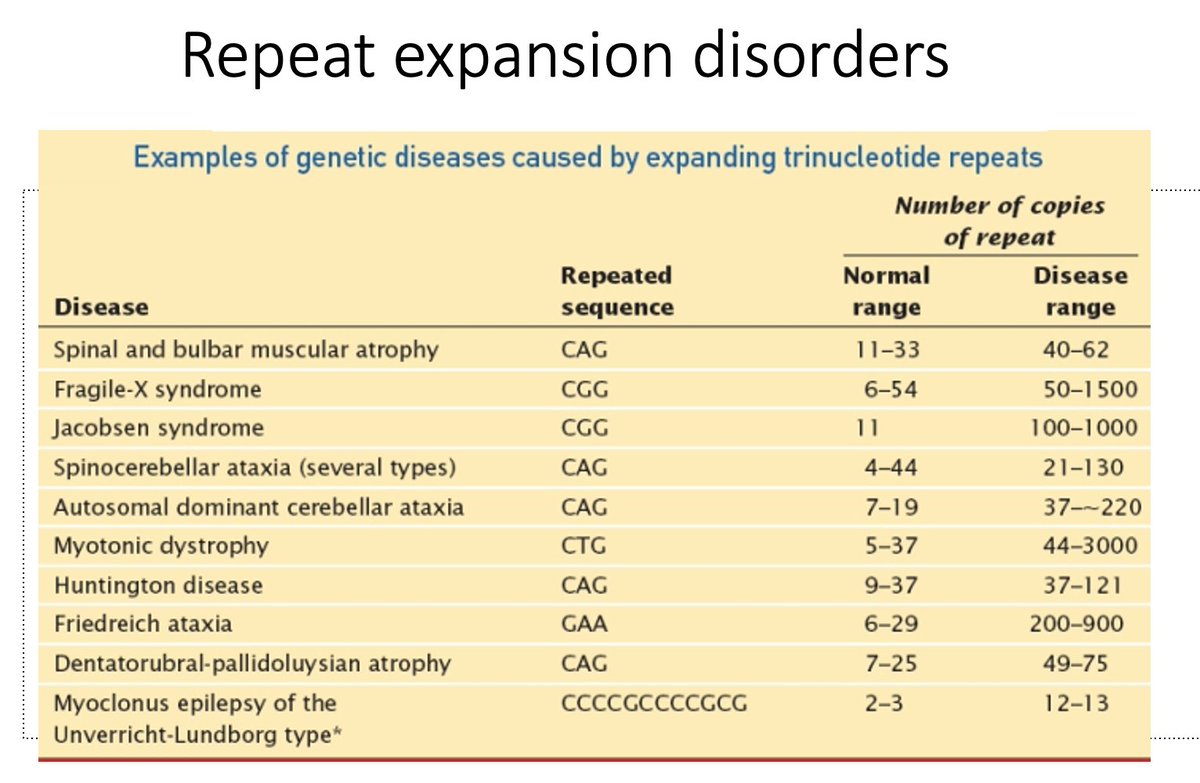
D. Triplet repeat testing
Testing for expansion disorders like Huntington disease, Fragile X, myotonic dystrophy, or many forms of cerebellar ataxia? The best sequencing will miss these mutations and you need to send for these conditions separately.
Testing for expansion disorders like Huntington disease, Fragile X, myotonic dystrophy, or many forms of cerebellar ataxia? The best sequencing will miss these mutations and you need to send for these conditions separately.

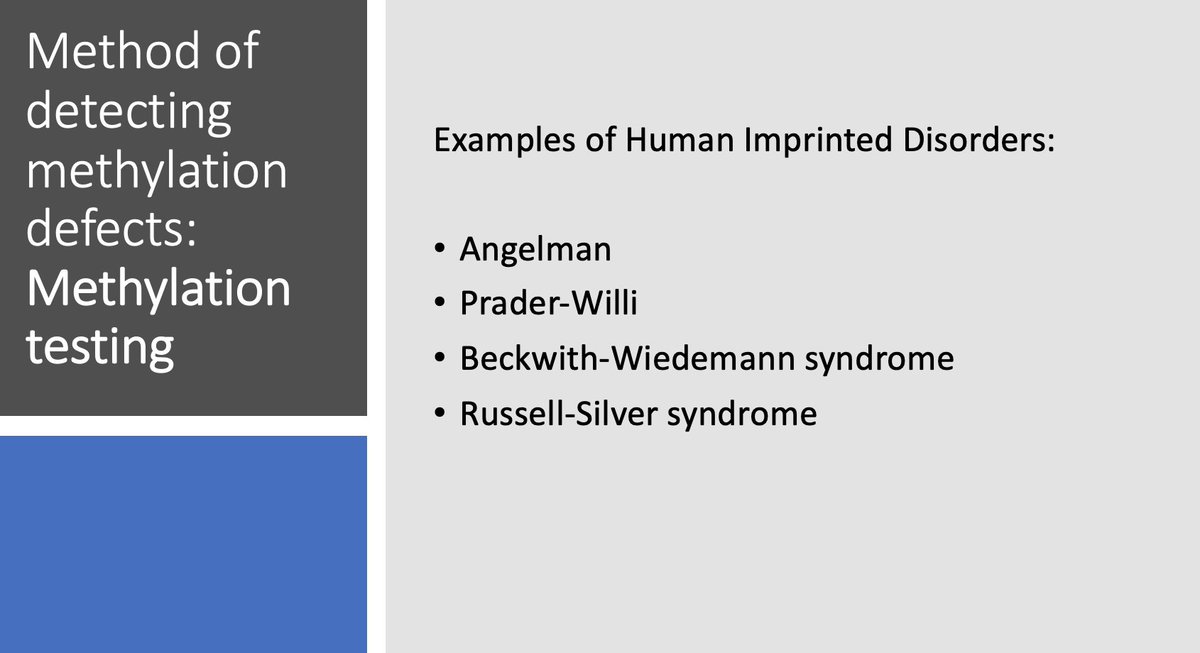
E. Methylation testing
How about Angelman and Prader-Willi? Where diseases can be caused not by changes to the sequence but by methylation defects of DNA? These can be missed on sequencing too. You need a methylation test.
How about Angelman and Prader-Willi? Where diseases can be caused not by changes to the sequence but by methylation defects of DNA? These can be missed on sequencing too. You need a methylation test.
F. Mitochondrial sequencing
Not all of our genes are found on those 46 chromosomes. We have some mitochondrial genes that we all inherited solely from our moms. These genes are tested using different methods. Mitochondrial sequencing.
Not all of our genes are found on those 46 chromosomes. We have some mitochondrial genes that we all inherited solely from our moms. These genes are tested using different methods. Mitochondrial sequencing.
Do you see how these gene-based tests mostly don't overlap? they are looking for different types of mutations in the genes.
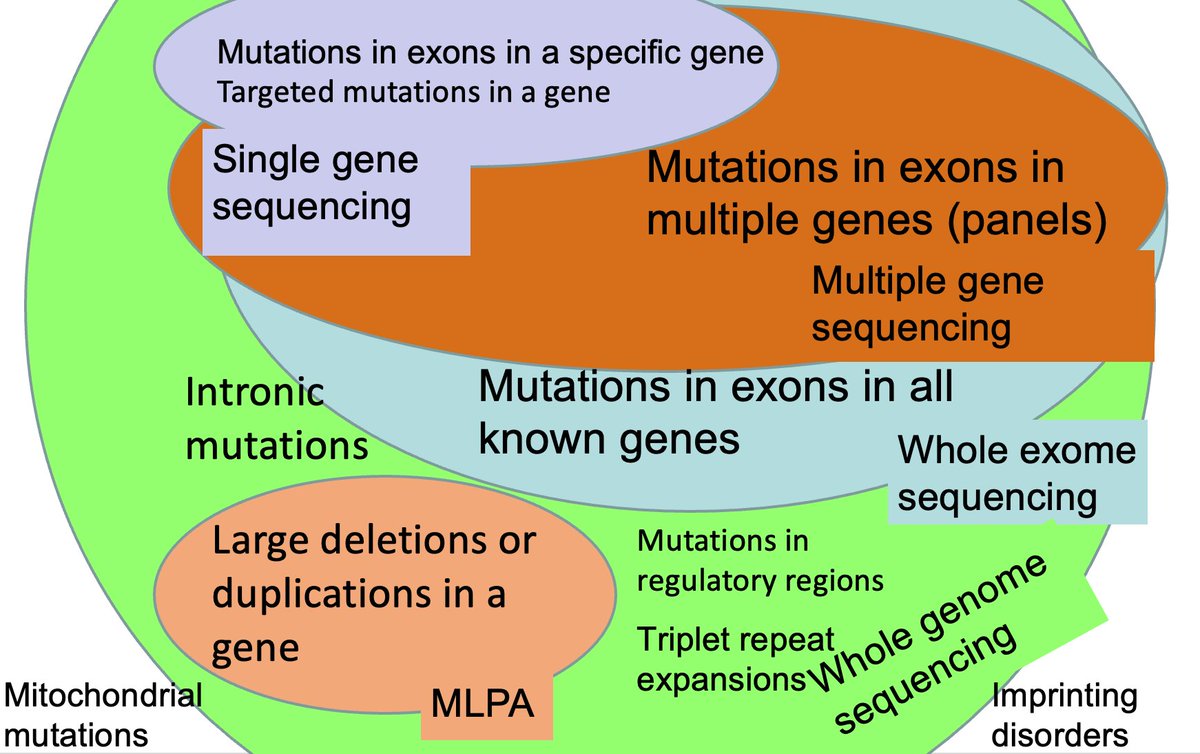
Okay, how about:
Whole Genome Sequencing?
This looks at chromosomal changes (remember those?) + sequences exons, non-coding regions, and triplet repeats all at once. It will still miss a few conditions though.
It's available, just not clinically everywhere yet.
Whole Genome Sequencing?
This looks at chromosomal changes (remember those?) + sequences exons, non-coding regions, and triplet repeats all at once. It will still miss a few conditions though.
It's available, just not clinically everywhere yet.
Sending the correct test is actually the easy part. Don't forget about the possible results you can receive and will have to interpret.
These apply mainly to microarray and sequencing tests. We recommend you counsel patients about these before you send them for a blood draw.
These apply mainly to microarray and sequencing tests. We recommend you counsel patients about these before you send them for a blood draw.

And since you've made it this far, don't forget about my hot tips, my fellow nerds!
https://twitter.com/HannanehF/status/1359752251959619584?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh