Fantasy commentary letter in Lancet (not a peer reviewed study)!
It's an unreasonable proposition for most countries like the UK to achieve elimination + constraints of reality negates claimed economic and liberty benefits if attempted...
1/
thelancet.com/journals/lance…
It's an unreasonable proposition for most countries like the UK to achieve elimination + constraints of reality negates claimed economic and liberty benefits if attempted...
1/
thelancet.com/journals/lance…
Despite pre-flight screening and quarantine Australia and New Zealand have failure rate of 4.8 per 100k travellers. SARS-COV-2 cases slip through!
2/
medrxiv.org/content/10.110…
2/
medrxiv.org/content/10.110…
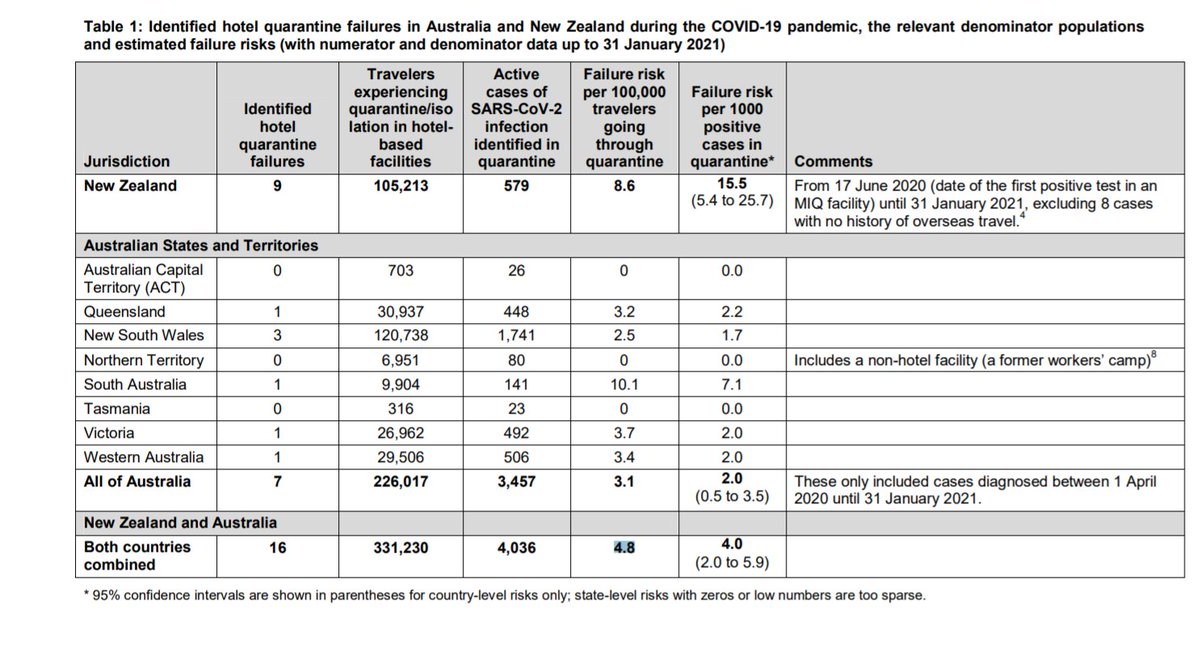
Those cases slipping through results in necessary lockdown (regional or state wise) to eliminate community transmission.
Up to January 31, 2021:
Australia 7 failures, with 1 causing 800 deaths
New Zealand 9 failures, 1 causing an outbreak of 3 deaths
more since
3/
Up to January 31, 2021:
Australia 7 failures, with 1 causing 800 deaths
New Zealand 9 failures, 1 causing an outbreak of 3 deaths
more since
3/
For the UK:
7k daily lorry drivers bring food +industrial supplies via channel
29k+ daily crossings of the Northern Ireland border
These flows could not conceivably be halted, nor quarantine pre-screened. Introduction rate >>4.8/100k depending on prevalence in ROI and EU
4/
7k daily lorry drivers bring food +industrial supplies via channel
29k+ daily crossings of the Northern Ireland border
These flows could not conceivably be halted, nor quarantine pre-screened. Introduction rate >>4.8/100k depending on prevalence in ROI and EU
4/
Flight quarantine to be as effective as AUS/NZ wd severely limit number of inward travellers ~20k per week. Hugely damaging to skilled workforce movements, reuniting families, unis.
Despite UK sealed borders as much as possible (300k+/week) = introduction rate >>15 per week
5/
Despite UK sealed borders as much as possible (300k+/week) = introduction rate >>15 per week
5/
Most would not seed community clusters (K dispersion) but enough would.
Community outbreaks aren't picked up early enough as most cases mild. Not until moderate illness detected typically, hospitalisation or death. That's too late, too large. To eliminate need to lock down.
6/
Community outbreaks aren't picked up early enough as most cases mild. Not until moderate illness detected typically, hospitalisation or death. That's too late, too large. To eliminate need to lock down.
6/
Given UK introduction rate and cluster seeding:
To achieve and maintain elimination an 'actual ZERO' Covid policy would require a permanent state of national lockdown (Aus Stage 4 equivalent to Level 4+schools closed in Eng) despite sealing borders!
7/
To achieve and maintain elimination an 'actual ZERO' Covid policy would require a permanent state of national lockdown (Aus Stage 4 equivalent to Level 4+schools closed in Eng) despite sealing borders!
7/
Geographic compactness and density of the UK/England would necessiciate lockdown be near national in scale to actually eliminate all seeded domestic SARS-COV-2 infections - similar to Aus States.
8/
8/
The effect of permanent Level 4 lockdown negates those economic and liberty gains supposed in the Lancet letter.
The scale of COVID cases, hospitalisations and deaths would be much less in this UK elimination counterfactual, but still much more than Aus/NZ...
9/
The scale of COVID cases, hospitalisations and deaths would be much less in this UK elimination counterfactual, but still much more than Aus/NZ...
9/
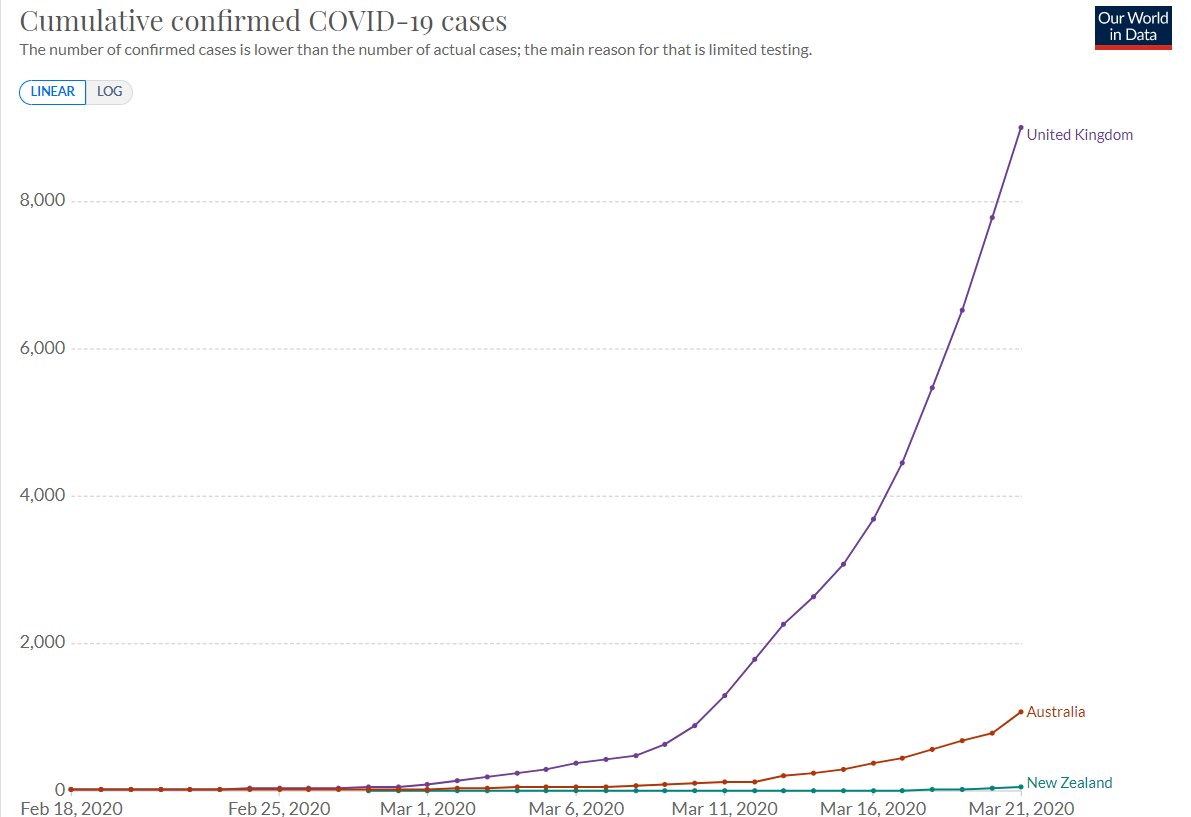
Aus/NZ did not move to elimination until after March 20th when they sealed borders.
The same geographic/economic connectivity and flows of peoples meant that UK outbreak was several orders of magnitude larger by then. UK 1st wave would have similar outcome by then.
10/
The same geographic/economic connectivity and flows of peoples meant that UK outbreak was several orders of magnitude larger by then. UK 1st wave would have similar outcome by then.
10/
Subsequent waves would have been much less damaging in terms of deaths with continual sporadic low level outbreaks despite lockdown.
But excess ~47k deaths from 1st wave would have resulted before the switch to elimination strategy at the same time as Aus/NZ.
11/
But excess ~47k deaths from 1st wave would have resulted before the switch to elimination strategy at the same time as Aus/NZ.
11/
This reasoning does not mean Aus/NZ should not have gone for elimination - actual zero covid.
They leveraged all their natural advantages w/ policies to achieve the best outcome for them in terms of health and GDP.
I wish all countries were as lucky as Australia.
12/
They leveraged all their natural advantages w/ policies to achieve the best outcome for them in terms of health and GDP.
I wish all countries were as lucky as Australia.
12/
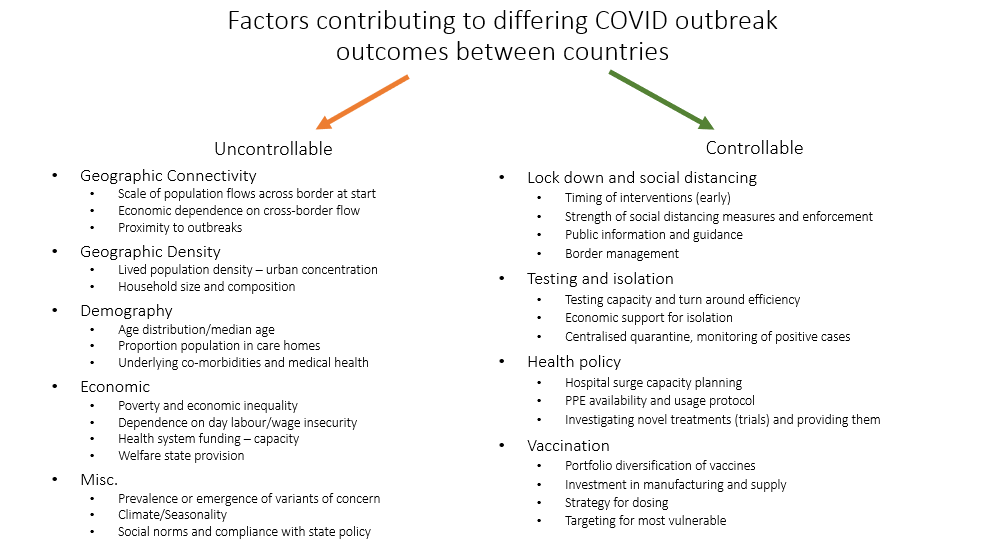
The reasons countries have serious covid outbreaks (infections or higher deaths rates) are multifactorial. Not all of them are under the control of public/health policy makers.
#coronacentrist manifesto👇
13/
#coronacentrist manifesto👇
13/
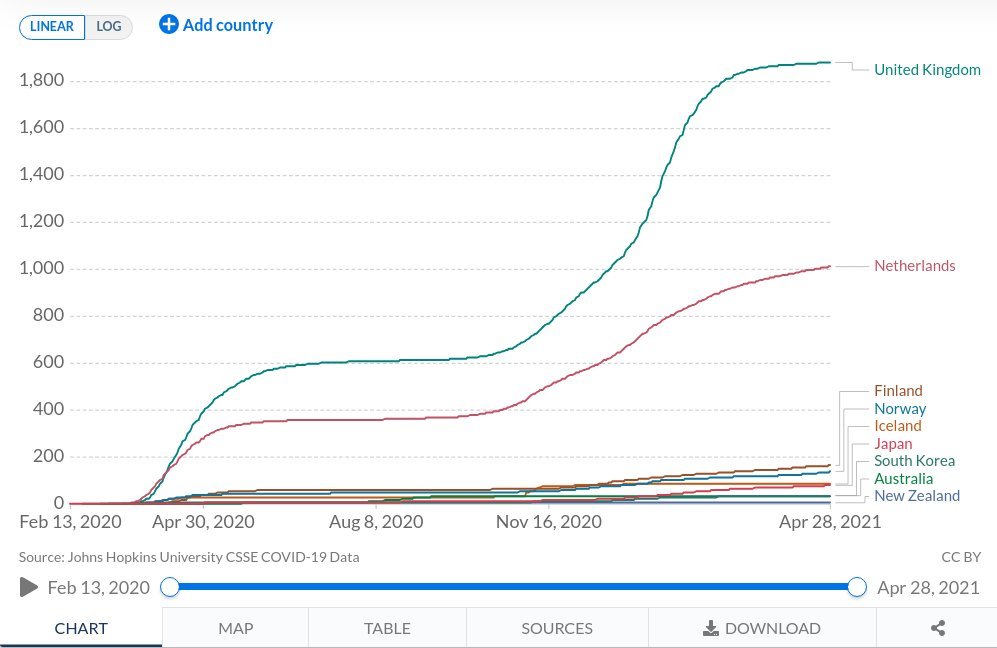
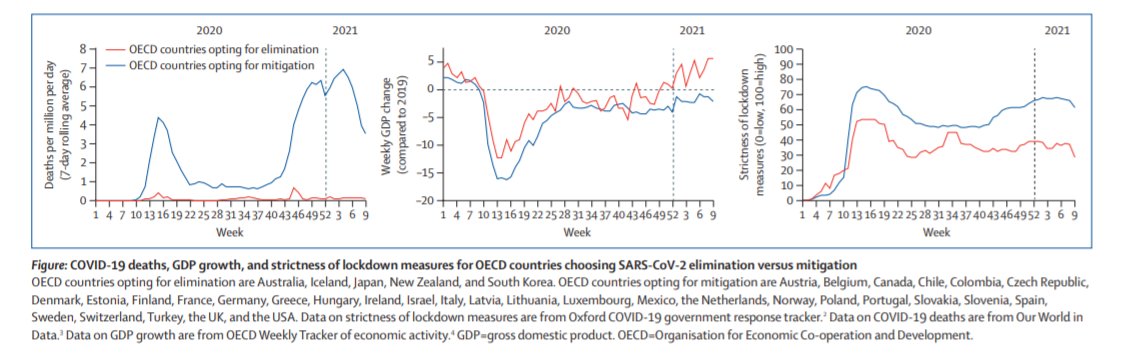
Lancet letter also mischaracterises countries like Japan as elimination- it's not- has successful suppression strategy (higher domestic case rate than UK now).
And bundles successful suppression countries (Nordics, Germany etc) from whom we can learn and less successful.
14/
And bundles successful suppression countries (Nordics, Germany etc) from whom we can learn and less successful.
14/
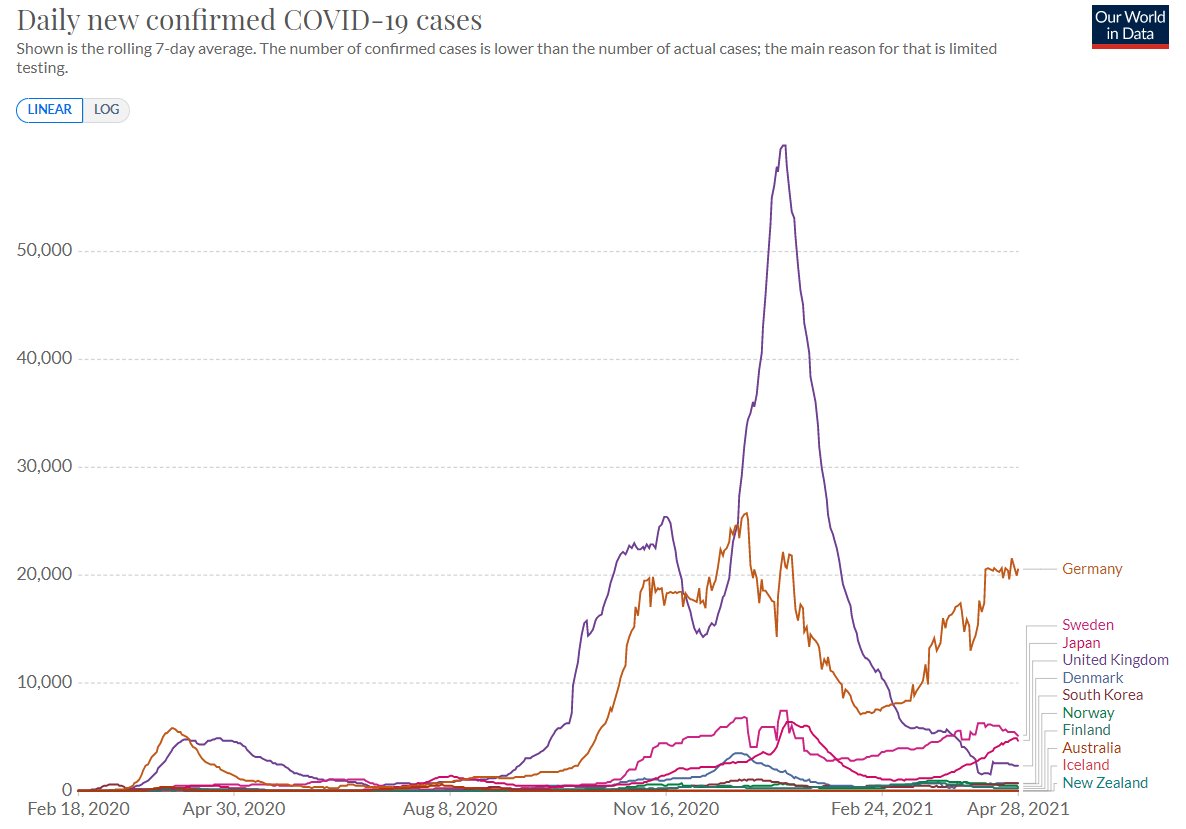
The range in what the suppression strategy involved, how successfully implemented, uncontrollable factors and resultant outcomes for deaths and GDP varied hugely in the 'suppression' countries. They are too mixed to lump together and analyse as one group.
15/
15/
P.S. Lancet comment on elimination contained this disclaimer
"our analysis does not prove a causal connection"
It's not serious analysis work, nor a basis for policy recommendation... ie be an isolated island w/ low cross border traffic (🇰🇷 included thanks to DMZ)
16/
"our analysis does not prove a causal connection"
It's not serious analysis work, nor a basis for policy recommendation... ie be an isolated island w/ low cross border traffic (🇰🇷 included thanks to DMZ)
16/
Summary:
Attempting an elimination strategy would have resulted in tens of thousands fewer deaths in UK, but it would have failed in definitional terms and required permanent national lockdown diminishing economic and liberty gains.
That would be an honest policy debate.
ENDS/
Attempting an elimination strategy would have resulted in tens of thousands fewer deaths in UK, but it would have failed in definitional terms and required permanent national lockdown diminishing economic and liberty gains.
That would be an honest policy debate.
ENDS/
An updated analysis to 31st March for Aus/NZ. Slightly higher failure rate and 2.3 reactive lockdowns per 100k travellers.
At the scale of UK cross border flows would be 7+ lockdowns per week if truly aiming for domestic elimination!
At the scale of UK cross border flows would be 7+ lockdowns per week if truly aiming for domestic elimination!
https://twitter.com/AdamJKucharski/status/1387877269708943371?s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh