Always a great study when tweeted out by Dr. Noakes - let's dive in.
✅2 cases of transmission from bus drivers to passengers up to more than 9 feet/ 3 meters.
✅Genomic confirmation
✅Airflow traced - please see Dr. Noakes original thread for commentary on the method used.
✅2 cases of transmission from bus drivers to passengers up to more than 9 feet/ 3 meters.
✅Genomic confirmation
✅Airflow traced - please see Dr. Noakes original thread for commentary on the method used.
https://twitter.com/CathNoakes/status/1388160910192168960
Limitations:
📌Facemask compliance unsure
📌Fomite possible. Not likely
📌Community transmission possible - but not likely
📌Facemask compliance unsure
📌Fomite possible. Not likely
📌Community transmission possible - but not likely

Two trips and two separate van drivers involved.
Both trips - windows closed, ventilation NOT on recirculate, heaters on medium fan.
First trip - 4 patients on 2-hour trips to and from the hospital on December 2, 2020. Driver tested +positive on December 3, 2020.
Van below.
Both trips - windows closed, ventilation NOT on recirculate, heaters on medium fan.
First trip - 4 patients on 2-hour trips to and from the hospital on December 2, 2020. Driver tested +positive on December 3, 2020.
Van below.

Driver had a high viral burden: 15.9
Driver and all passengers wore cloth facemasks and only interacted during boarding and transportation.
Driver and all passengers wore cloth facemasks and only interacted during boarding and transportation.

Second trip - The second driver transported 3 patients on the same 2-hour trip in the same van on
January 23, 2021, the day his symptoms began.
Van below.
January 23, 2021, the day his symptoms began.
Van below.

Driver viral load was high - 24.
Driver was not in a mask, but the passengers were.
Driver was not in a mask, but the passengers were.

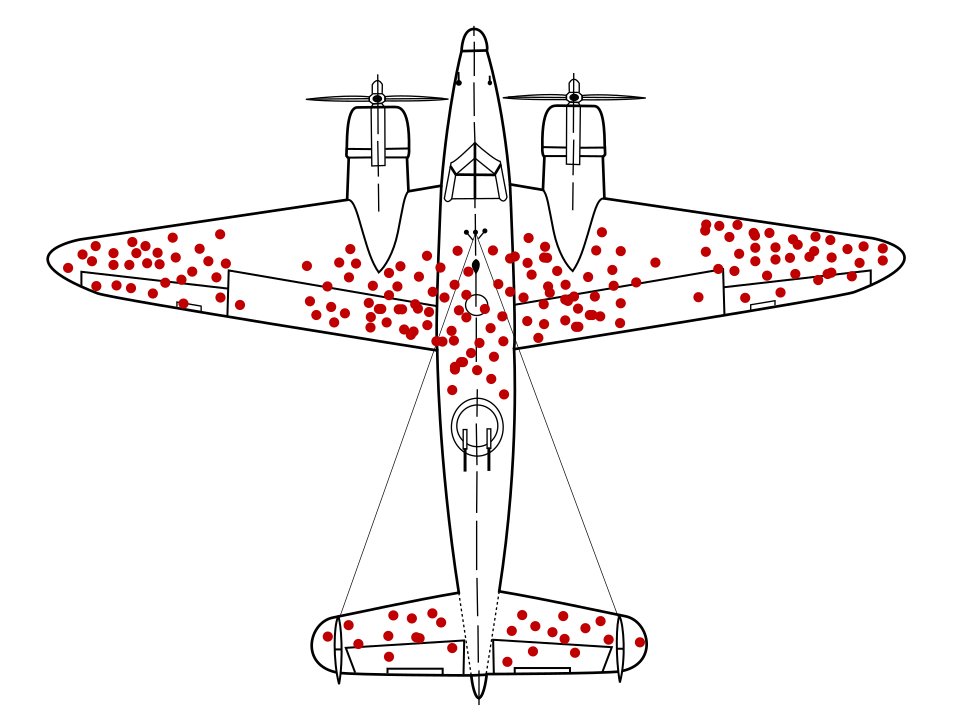
What everyone is most interested in - airflow tracing.
Heater on? Smoke released from the driver seat at headrest height rose and flowed toward the back of the van.
When heater and fans were off, no "microspheres" were recovered from the seats or air.
Next tweet method...
Heater on? Smoke released from the driver seat at headrest height rose and flowed toward the back of the van.
When heater and fans were off, no "microspheres" were recovered from the seats or air.
Next tweet method...


I don't remember seeing this exact technique before in any of the studies I've read. Not saying it's not valid at all. Just haven't seen it.

Contact Tracing Method

Genomic Method.

Our take-aways?
👉 #CoVidIsAirborne.
👉 #BetterMasks are necessary.
👉 If you open diagonal windows, you can create an air curtain. Like in this case, passenger and the window directly behind the driver.
In this case, that last bullet point was not possible due to passenger
👉 #CoVidIsAirborne.
👉 #BetterMasks are necessary.
👉 If you open diagonal windows, you can create an air curtain. Like in this case, passenger and the window directly behind the driver.
In this case, that last bullet point was not possible due to passenger
windows not being able to be opened.
H/T @linseymarr for the air curtain suggestion about 1 million pandemic years ago!
H/T @linseymarr for the air curtain suggestion about 1 million pandemic years ago!
• • •
Missing some Tweet in this thread? You can try to
force a refresh