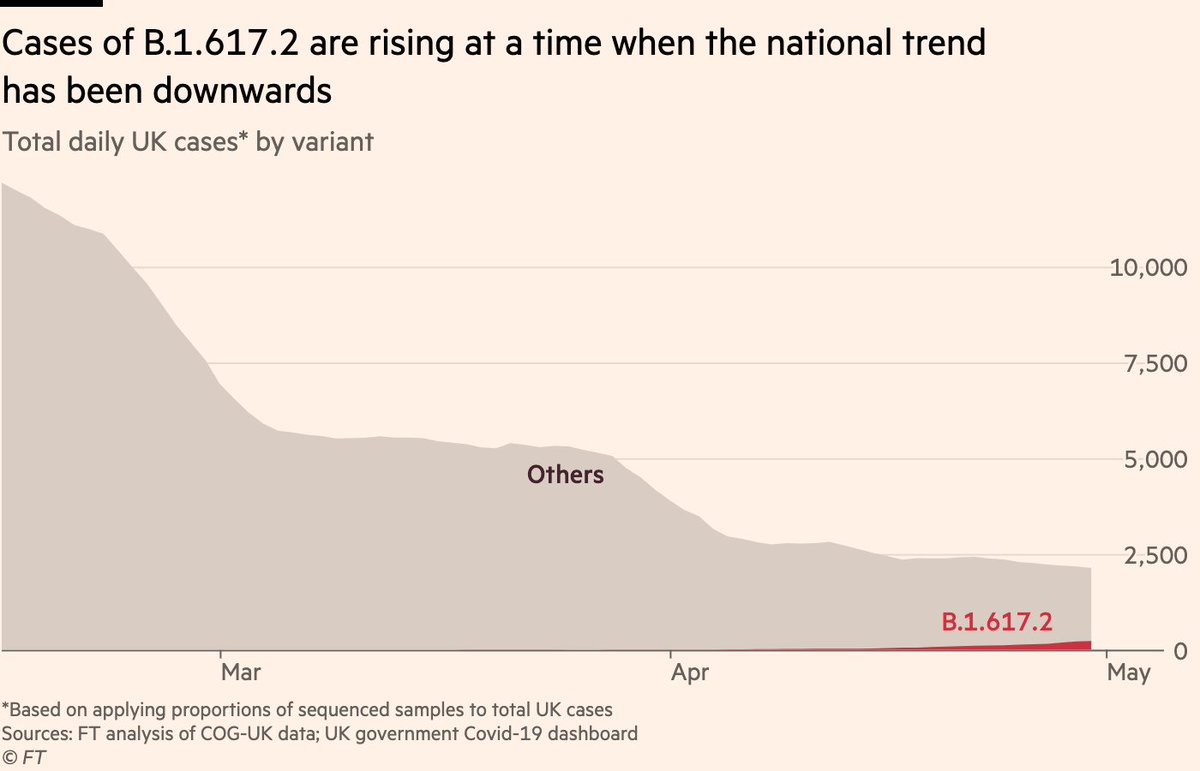
NEW: time for a proper thread on B.1.617.2, the subtype of the Indian variant that has been moved to "variant of concern" today by Public Health England.
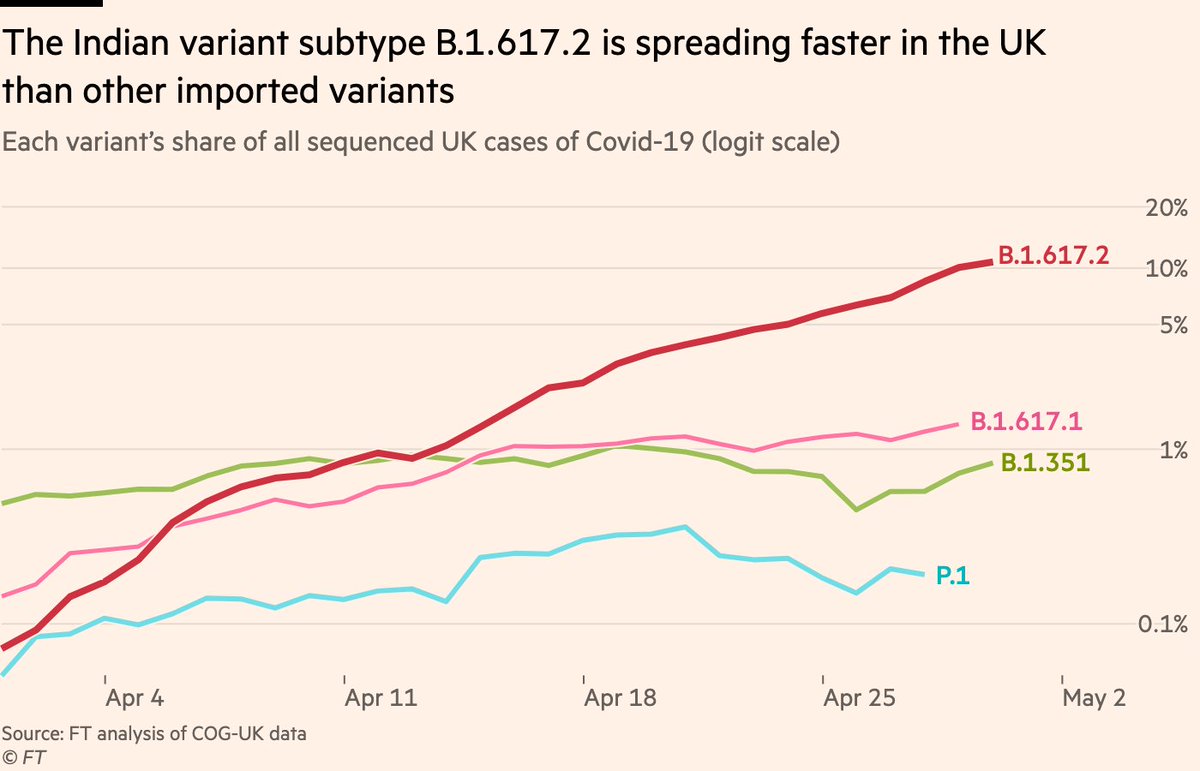
First, it’s clear case numbers from this lineage are growing faster than other imported variants have done in the UK.
First, it’s clear case numbers from this lineage are growing faster than other imported variants have done in the UK.
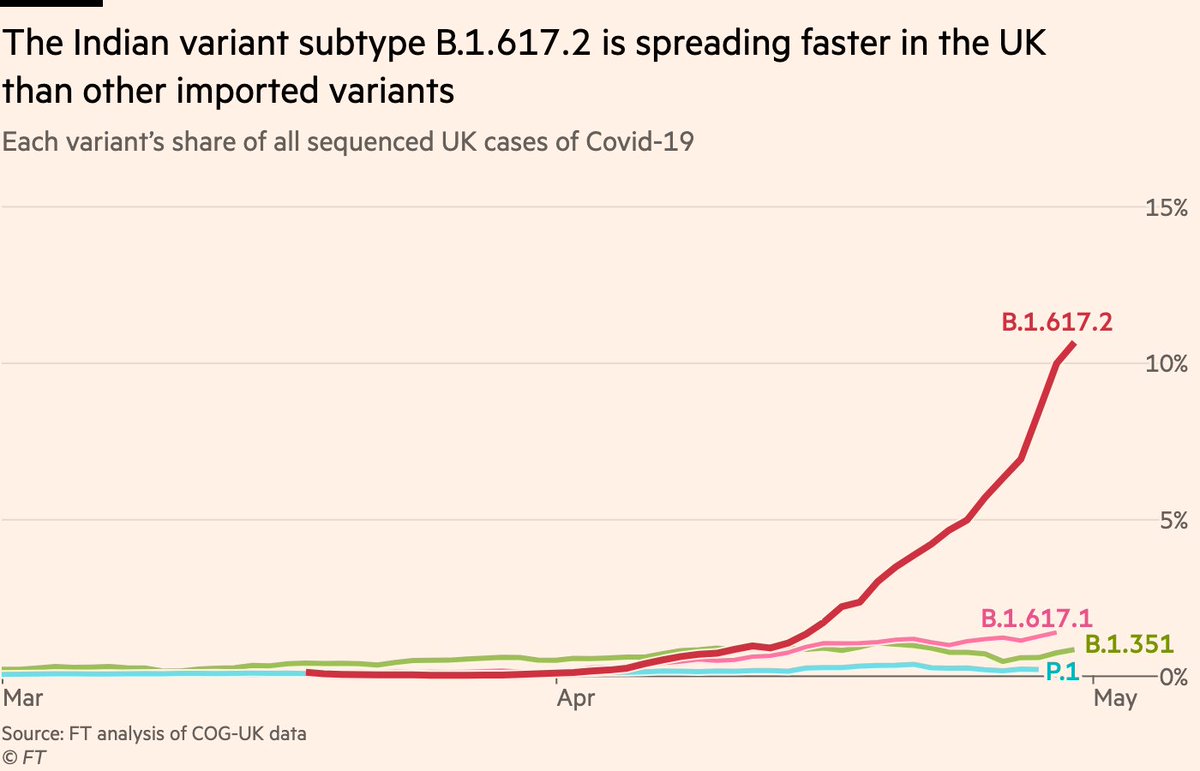
Here’s the same thing on a logit scale (HT @trvrb), which makes it easier to compare growth rates.
As we can see, B.1.617.2 is on a fairly steady upward trajectory, which other variants failed to achieve.
As we can see, B.1.617.2 is on a fairly steady upward trajectory, which other variants failed to achieve.
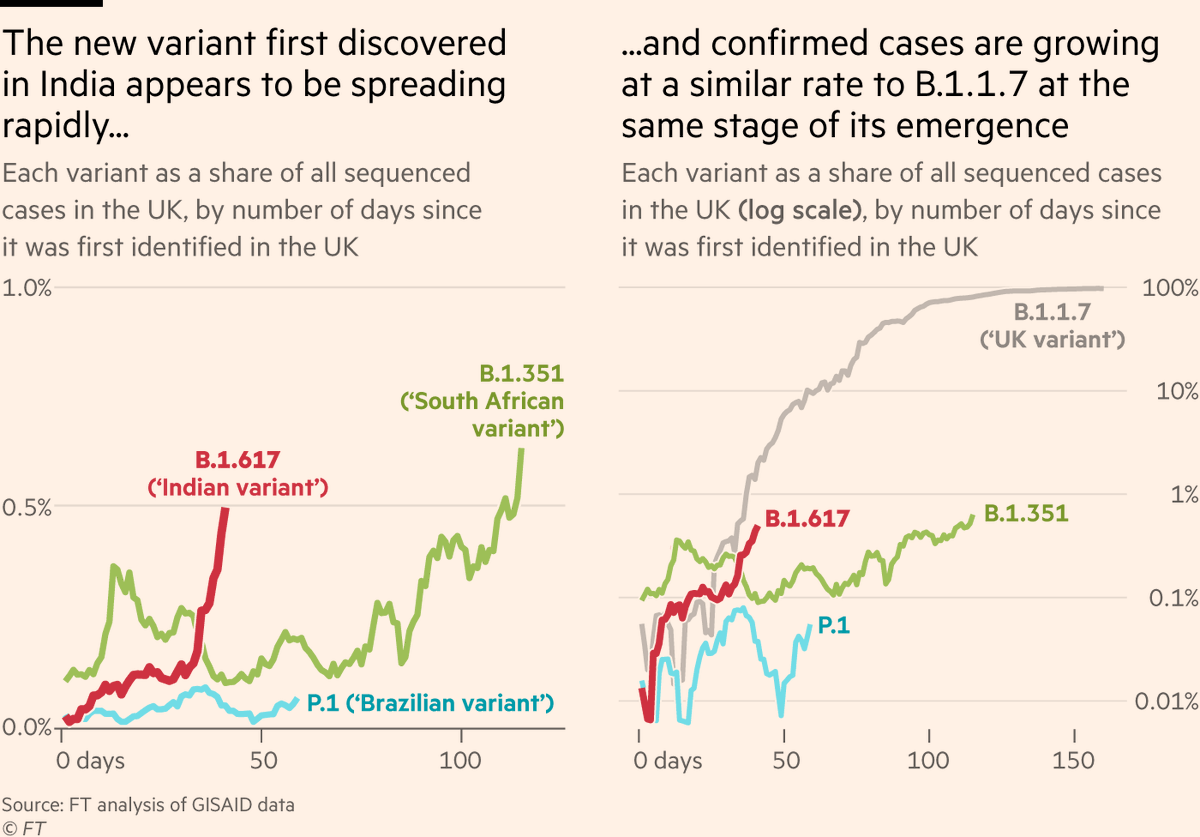
So we know its trajectory looks different to the other imported variants, but that doesn’t tell us enough. We need a better benchmark: how does its growth compare to B.1.1.7 at the same stage of its emergence?
Remarkably similar, it turns out:
Remarkably similar, it turns out:
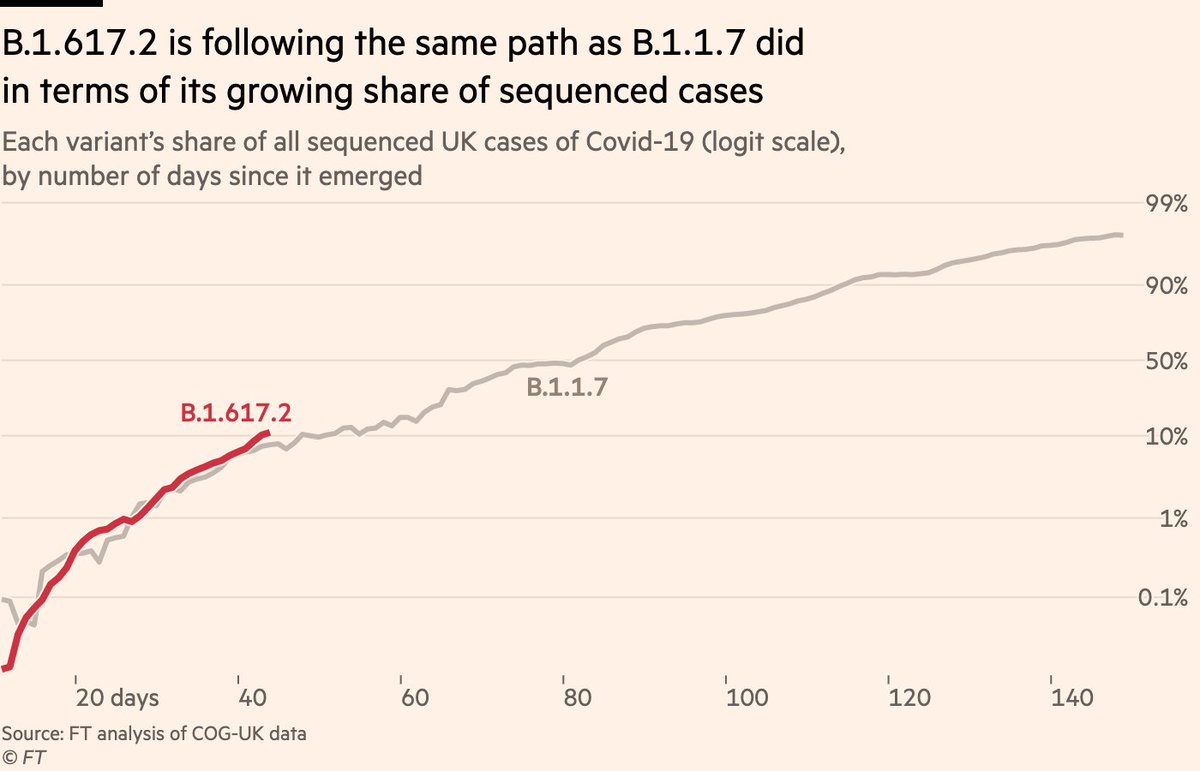
In terms of its share of all sequenced UK cases, B.1.617.2 is following ~exactly the same path as B.1.1.7 did last year.
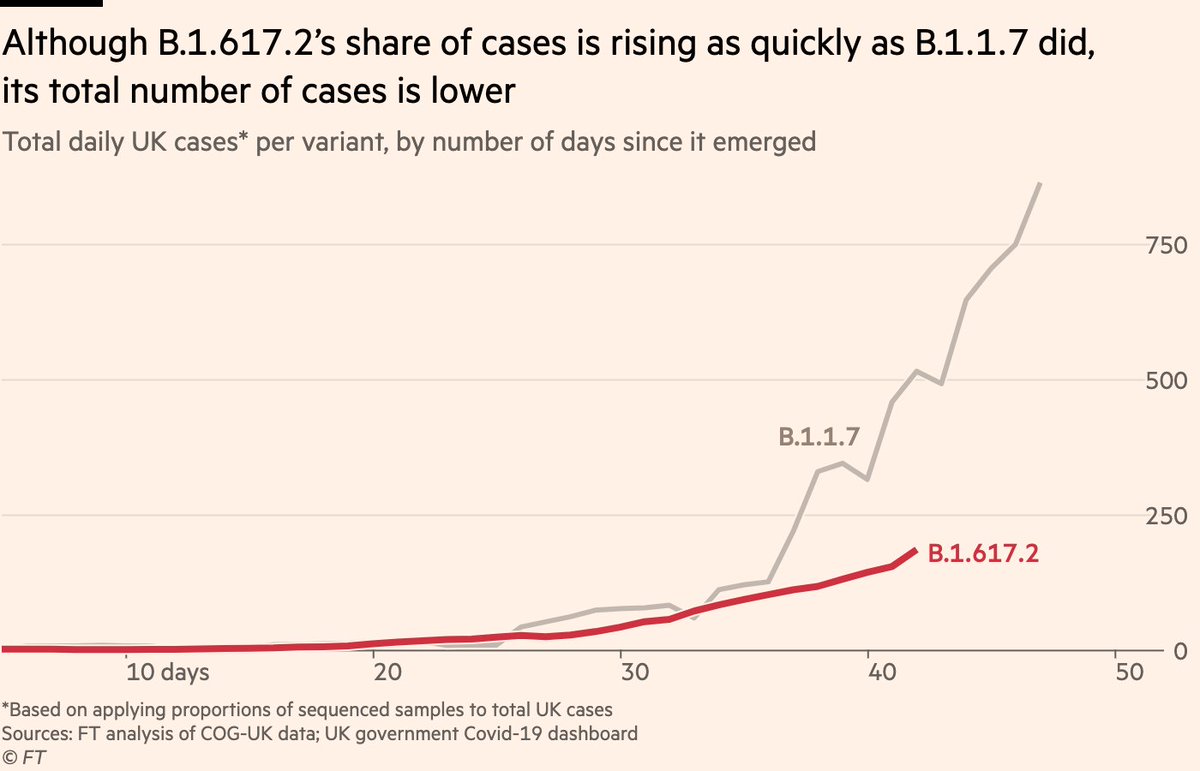
But there’s a caveat here, and it’s a double-edged caveat.
But there’s a caveat here, and it’s a double-edged caveat.
Because overall UK case numbers are much lower today than they were last November, the same % of cases is a smaller number.
If we map those %s onto total UK cases, we see there are much fewer new B.1.617. 2 infections today than there were with B.1.1.7 at the same point.
If we map those %s onto total UK cases, we see there are much fewer new B.1.617. 2 infections today than there were with B.1.1.7 at the same point.
And indeed, if we plot the same thing on a log scale, there are also signs B.1.617.2 may be following a slightly shallower ascent than B.1.1.7, too.
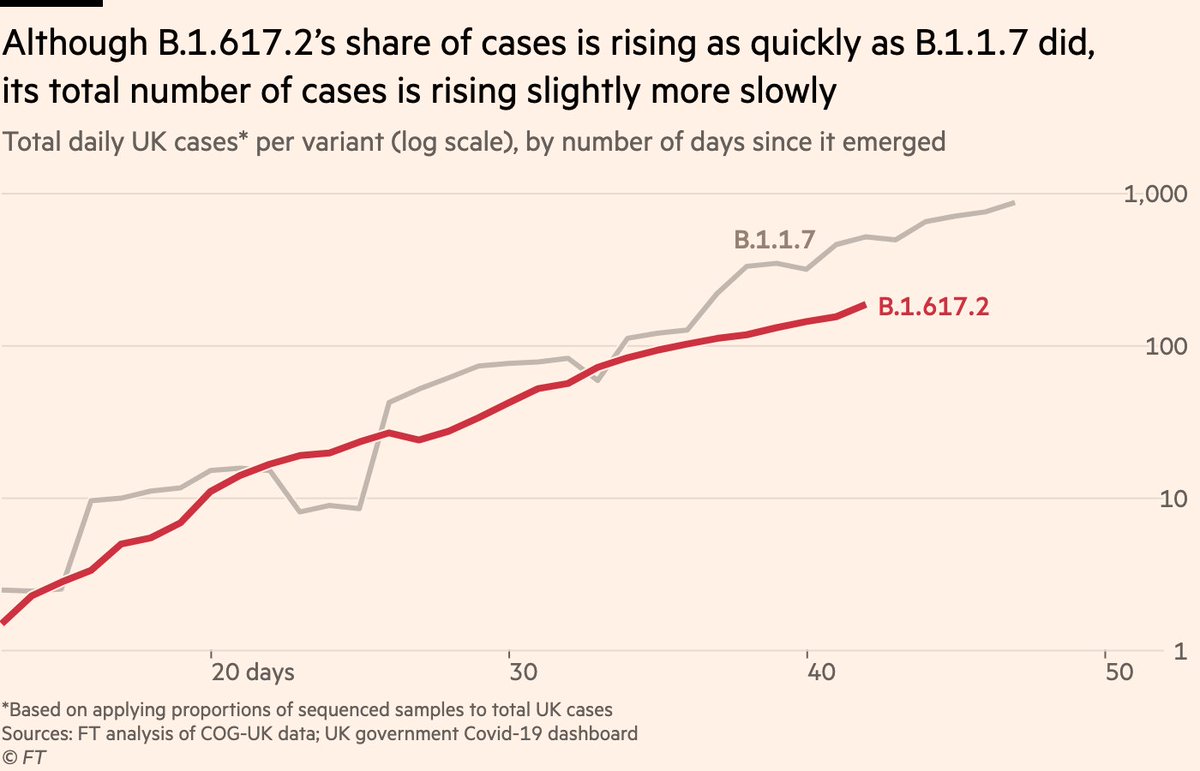
But the flip-side of this is, B.1.1.7 was growing when there was more social mixing. Conditions were favourable to transmission.
Numbers of B.1.617.2 are rising at a time of less mixing. This has led some to worry that it could be more transmissible (but we don’t yet know this).
Numbers of B.1.617.2 are rising at a time of less mixing. This has led some to worry that it could be more transmissible (but we don’t yet know this).
So how should we think about all of this?
First, there’s the data itself: it’s critical that we know how many of the B.1.617.2 cases are second-generation cases from returning travellers, and how many are genuine community spread.
Today PHE said almost half are travel-related.
First, there’s the data itself: it’s critical that we know how many of the B.1.617.2 cases are second-generation cases from returning travellers, and how many are genuine community spread.
Today PHE said almost half are travel-related.
All returning travellers have their tests sequenced, so we know this inflates numbers for B.1.617.2.
If national trend is downward, and you have a glut of travellers returning from India, the imported cases (and their secondary cases) alone could artificially imply rapid growth.
If national trend is downward, and you have a glut of travellers returning from India, the imported cases (and their secondary cases) alone could artificially imply rapid growth.
Hopefully we keep getting breakdowns of how many were linked to returning travellers and how many were not. In the absence of that, it’s a case of wait and see.
It was several weeks after this point that B.1.1.7 really took off. That may happen with B.1.617.2, or it may not.
It was several weeks after this point that B.1.1.7 really took off. That may happen with B.1.617.2, or it may not.

So that’s the issue with the data itself, but more important is what all of this means in the context of the vaccines.
And here, there are lots of reasons to be optimistic:
And here, there are lots of reasons to be optimistic:
First, B.1.617.2 does not have the E484Q mutation, which has been linked to immune escape.
Among its mutations is L452R, which @GuptaR_lab has found to be less immune-evasive than the mutations found in e.g the Brazilian and South African variants
Among its mutations is L452R, which @GuptaR_lab has found to be less immune-evasive than the mutations found in e.g the Brazilian and South African variants
https://twitter.com/GuptaR_lab/status/1388422662595219459
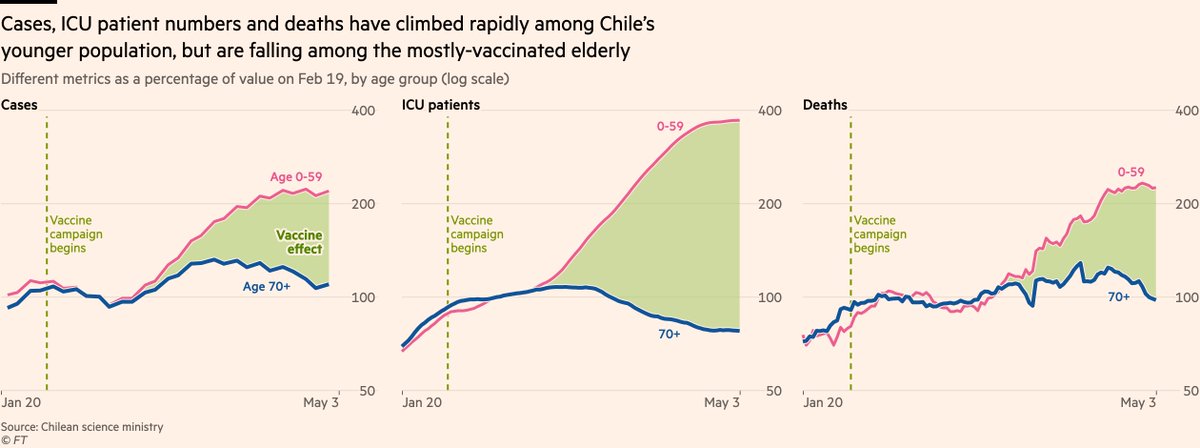
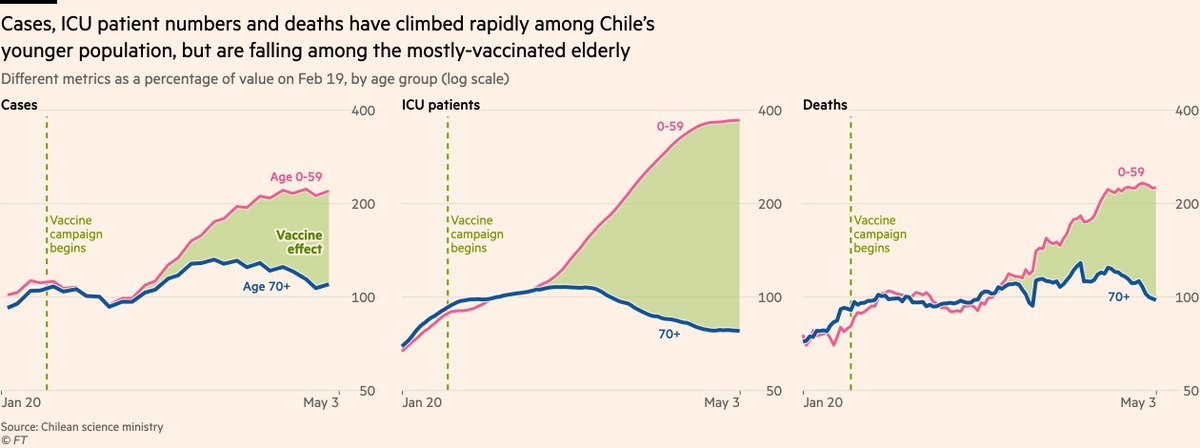
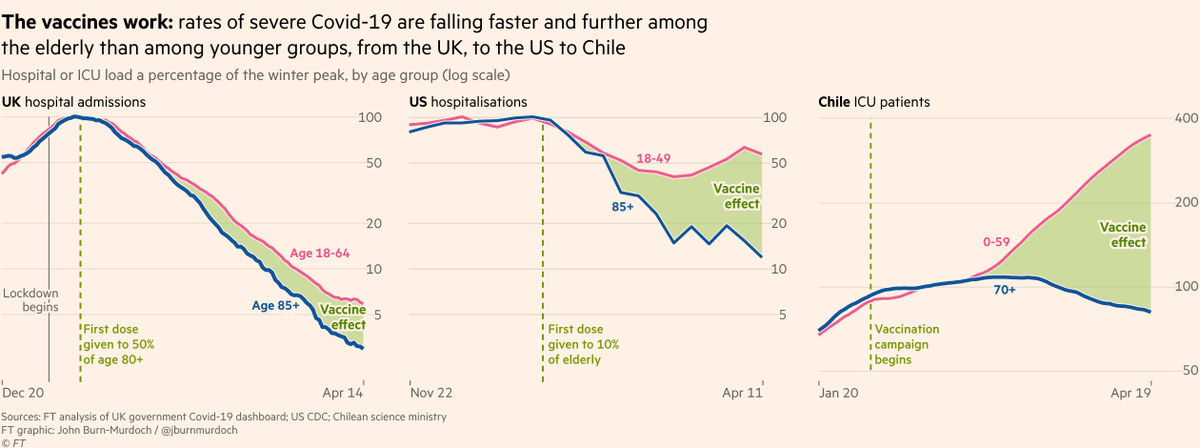
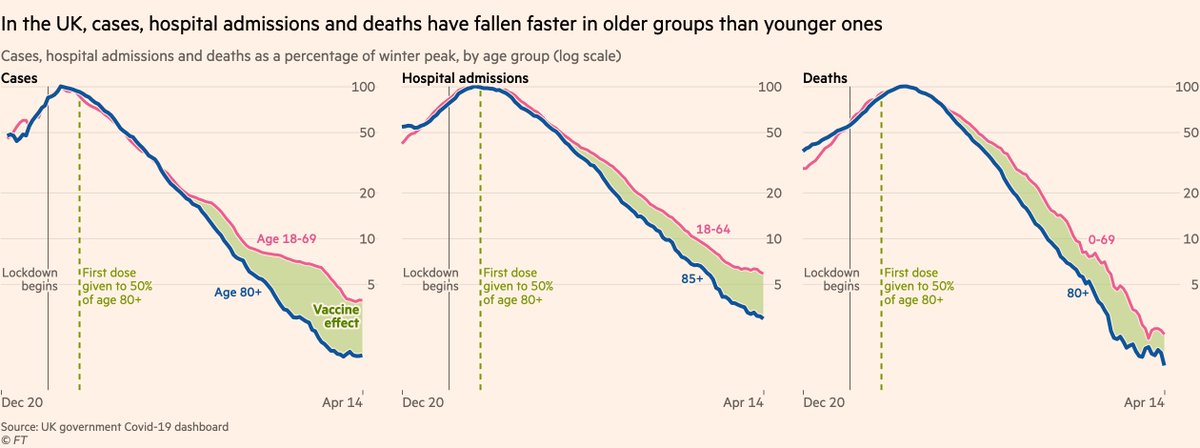
And second, the data we do have on people being infected with B.1.617.2 after receiving the vaccine is — despite claims to the contrary — very reassuring.
Even among the most vulnerable populations, infections are not turning into severe illness or death
Even among the most vulnerable populations, infections are not turning into severe illness or death
https://twitter.com/DevanSinha/status/1390388896433942544
This is strongly supportive of the last point about mutations & immune escape:
If (and it remains an if) B.1.617.2 is found to be more transmissible than other variants, it doesn’t look like vaccines will struggle to protect infected people from getting seriously ill.
If (and it remains an if) B.1.617.2 is found to be more transmissible than other variants, it doesn’t look like vaccines will struggle to protect infected people from getting seriously ill.
As @mugecevik told @AnnaSophieGross in our story, "Right now the most important thing is that the vaccines are working against this variant".
And it really is as simple as that until we learn more.
As I’ve been saying, keep *watching*, but don’t keep *worrying*.
And it really is as simple as that until we learn more.
As I’ve been saying, keep *watching*, but don’t keep *worrying*.
Here’s our full story: ft.com/content/8e1347…
And here’s @PHE_uk’s report today gov.uk/government/new…
And here’s @PHE_uk’s report today gov.uk/government/new…
Final comments:
I’ve deliberately included the "numbers are rising!" charts alongside the caveats about why that is not necessarily reason to worry. I think it’s important to show the raw data, even if there are many reasons to take it with a pinch of salt.
I’ve deliberately included the "numbers are rising!" charts alongside the caveats about why that is not necessarily reason to worry. I think it’s important to show the raw data, even if there are many reasons to take it with a pinch of salt.
I also want people to realise 2 things can both be true: numbers rising, and the situation not necessarily being scary.
It’s not either or. If someone shows you a scary chart of rising numbers, ask whether it really is scary given what else we know (and hey, perhaps it will be).
It’s not either or. If someone shows you a scary chart of rising numbers, ask whether it really is scary given what else we know (and hey, perhaps it will be).
I’ll continue to share as much information as I have on B.1.617.2 as the picture becomes clearer.
As ever, feel free to get in touch with questions, comments etc.
As ever, feel free to get in touch with questions, comments etc.
• • •
Missing some Tweet in this thread? You can try to
force a refresh