
1/
📢Tweetorial alert!
Hey #medtwitter! Have you checked out @TheskeletonKG latest case - a rare cause of hypokalemia?
renalfellow.org/2021/05/22/ske…
Let's go through it together
#NSMC #FOAMed #NephTwitter @NSMCInternship
📢Tweetorial alert!
Hey #medtwitter! Have you checked out @TheskeletonKG latest case - a rare cause of hypokalemia?
renalfellow.org/2021/05/22/ske…
Let's go through it together
#NSMC #FOAMed #NephTwitter @NSMCInternship
2/
A 32-year-old woman, presented to the clinic with B/L lower extremity weakness & upper limb cramping for 2 weeks. Motor power 3/5 in lower limbs & 4/5 in upper limbs. B/L ankle & knee jerk reflexes were absent. She had 1 such episode in the past which recovered spontaneously.
A 32-year-old woman, presented to the clinic with B/L lower extremity weakness & upper limb cramping for 2 weeks. Motor power 3/5 in lower limbs & 4/5 in upper limbs. B/L ankle & knee jerk reflexes were absent. She had 1 such episode in the past which recovered spontaneously.
3/
She denied using any medications before the onset of symptoms. She had no family history of kidney disease. Her labs showed ⏬K⏬Mg, normal TSH and negative ANA. USG of the abdomen was normal.
She denied using any medications before the onset of symptoms. She had no family history of kidney disease. Her labs showed ⏬K⏬Mg, normal TSH and negative ANA. USG of the abdomen was normal.

4/
⚠️ Before evaluating hypokalemia, life threatening complications such as arrhythmias and paralysis should be looked for. If present, it should be treated with IV potassium(K) & magnesium(Mg)
⚠️ Before evaluating hypokalemia, life threatening complications such as arrhythmias and paralysis should be looked for. If present, it should be treated with IV potassium(K) & magnesium(Mg)
5/
The next step in evaluating hypokalemia is differentiating kidney K wasting from other causes.
📌A urine K/Cr ratio >15 mEq/g suggests urinary losses.
⚡️A K/Cr ratio of 23 mEq/g in this patient identifies kidney as the culprit of K loss.
The next step in evaluating hypokalemia is differentiating kidney K wasting from other causes.
📌A urine K/Cr ratio >15 mEq/g suggests urinary losses.
⚡️A K/Cr ratio of 23 mEq/g in this patient identifies kidney as the culprit of K loss.

6/
With a BP of 106/70 mm Hg, we checked the acid base status next. The presence of metabolic alkalosis narrowed down the diagnosis to either vomiting/ diuretic use/ Gitelman syndrome (GS) or Bartter syndrome(BS)
With a BP of 106/70 mm Hg, we checked the acid base status next. The presence of metabolic alkalosis narrowed down the diagnosis to either vomiting/ diuretic use/ Gitelman syndrome (GS) or Bartter syndrome(BS)

7/
📌Urine chloride levels <10 mmol/L indicate GI losses.
📌Urine Ca/Cr ratio <0.07 mg/mg is suggestive of hypocalciuria & is seen in GS & thiazide use. A ratio >0.20 is seen in Bartter syndrome & with loop diuretics suggesting hypercalciuria.
📌Urine chloride levels <10 mmol/L indicate GI losses.
📌Urine Ca/Cr ratio <0.07 mg/mg is suggestive of hypocalciuria & is seen in GS & thiazide use. A ratio >0.20 is seen in Bartter syndrome & with loop diuretics suggesting hypercalciuria.

8/
⚡️Increased urine chloride excretion of 80 mEq/L and a Ca/Cr ratio of 0.04 mg/mg in our patient, with no history of thiazide use narrowed down our diagnosis to GS.
⚠️ Be careful of those units when working on those computations! ⚠️
⚡️Increased urine chloride excretion of 80 mEq/L and a Ca/Cr ratio of 0.04 mg/mg in our patient, with no history of thiazide use narrowed down our diagnosis to GS.
⚠️ Be careful of those units when working on those computations! ⚠️

9/
Why do we think it's Gitelman syndrome? She had
🔸Hypokalemia
🔸Hypomagnesemia
🔸Normal BP
🔸Metabolic alkalosis
🔸Hypocalciuria
Why do we think it's Gitelman syndrome? She had
🔸Hypokalemia
🔸Hypomagnesemia
🔸Normal BP
🔸Metabolic alkalosis
🔸Hypocalciuria
10/
🧬GS is a rare autosomal recessive salt-losing tubulopathy with a prevalence of 1- 10 in 40,000, estimated to be higher in Asians. It occurs due to inactivating mutations in the SLC12A3 gene that encodes thiazide-sensitive sodium-chloride cotransporter in the distal tubule.
🧬GS is a rare autosomal recessive salt-losing tubulopathy with a prevalence of 1- 10 in 40,000, estimated to be higher in Asians. It occurs due to inactivating mutations in the SLC12A3 gene that encodes thiazide-sensitive sodium-chloride cotransporter in the distal tubule.

11/
Patients with GS usually present in late childhood/ early adulthood. Although the majority of them have mild or nonspecific symptoms, severe life-threatening complications can rarely occur @goKDIGO @Kidney_Int
kidney-international.org/article/S0085-…
Patients with GS usually present in late childhood/ early adulthood. Although the majority of them have mild or nonspecific symptoms, severe life-threatening complications can rarely occur @goKDIGO @Kidney_Int
kidney-international.org/article/S0085-…

12/
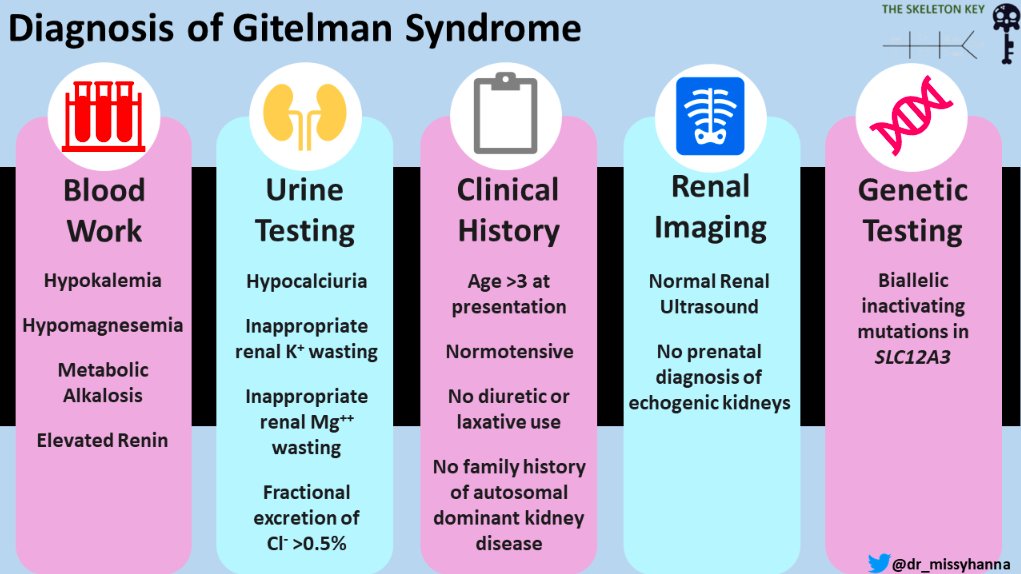
The criteria to diagnose Gitelman syndrome includes clinical, biochemical parameters often supported by genetic testing.
The criteria to diagnose Gitelman syndrome includes clinical, biochemical parameters often supported by genetic testing.
13/
The differential diagnosis of GS include
The differential diagnosis of GS include
14/
All of the above!
📌Thiazide use is associated with variable Cl excretion & a positive urine assay for diuretics
📌cBS occurs at a younger age, with failure to thrive, polyuria with usually normal Mg levels
All of the above!
📌Thiazide use is associated with variable Cl excretion & a positive urine assay for diuretics
📌cBS occurs at a younger age, with failure to thrive, polyuria with usually normal Mg levels
15/
📌HNF1B mutations associated with MODY, early CKD, family history, abnormal liver enzymes, renal/urogenital malformations
📌KCNJ10 mutations present with EAST syndrome
📌HNF1B mutations associated with MODY, early CKD, family history, abnormal liver enzymes, renal/urogenital malformations
📌KCNJ10 mutations present with EAST syndrome
16/
Treatment includes
🔹Electrolyte replacement - K & Mg, preferably Cl salts
🔹K & Mg rich food
🔹Liberal salt intake
🔹In persistent hypokalemia, K sparing diuretics, RAASi, NSAIDS may be used with caution
🎯Target K levels- 3.0 mEq/L
🎯Target Mg levels- 1.4 mg/dl @goKDIGO
Treatment includes
🔹Electrolyte replacement - K & Mg, preferably Cl salts
🔹K & Mg rich food
🔹Liberal salt intake
🔹In persistent hypokalemia, K sparing diuretics, RAASi, NSAIDS may be used with caution
🎯Target K levels- 3.0 mEq/L
🎯Target Mg levels- 1.4 mg/dl @goKDIGO

17/
Side effects of the drugs include abdominal pain, diarrhoea & gastritis. Patient should be followed up regularly til near normal/stable levels of K & Mg is achieved. At least an annual follow up is recommended thereafter, to monitor potential complications & disease evolution
Side effects of the drugs include abdominal pain, diarrhoea & gastritis. Patient should be followed up regularly til near normal/stable levels of K & Mg is achieved. At least an annual follow up is recommended thereafter, to monitor potential complications & disease evolution
18/
Long term management include
📌Educating patients & caregivers about GS & its outcome
📌Individualised measures to improve school/work performance & QOL
⭐Various groups help create awareness & offer support to pts with GS @gitelmansuk gitelmansyndrome.co.uk
Long term management include
📌Educating patients & caregivers about GS & its outcome
📌Individualised measures to improve school/work performance & QOL
⭐Various groups help create awareness & offer support to pts with GS @gitelmansuk gitelmansyndrome.co.uk

19/
To Summarize
🔑GS presents with⏬K⏬Mg, met alkalosis, hypocalciuria, normal BP
🔑Urine K/Cr ratio >15 mEq/g= kidney K loss
🔑Urine Ca/Cr ratio <0.07 mg/mg= GS/thiazides & >0.20= BS/loop diuretic
🔑Bialleic inactivating mutation of SLC12A3= GS
🔑Treatment-K & Mg replacement
To Summarize
🔑GS presents with⏬K⏬Mg, met alkalosis, hypocalciuria, normal BP
🔑Urine K/Cr ratio >15 mEq/g= kidney K loss
🔑Urine Ca/Cr ratio <0.07 mg/mg= GS/thiazides & >0.20= BS/loop diuretic
🔑Bialleic inactivating mutation of SLC12A3= GS
🔑Treatment-K & Mg replacement
20/
Check out this fabulous VA by @NSMC intern @nephromythri Thank you to the @TheSkeletonKG members,@dr_missyhanna @SRameshMD for helping me put this case together! Til next month! 🏴☠️
Check out this fabulous VA by @NSMC intern @nephromythri Thank you to the @TheSkeletonKG members,@dr_missyhanna @SRameshMD for helping me put this case together! Til next month! 🏴☠️

• • •
Missing some Tweet in this thread? You can try to
force a refresh


