Lead researcher for CDC's Vaccine Breakthrough Team has confirmed that fully-vaxed patients who are hospitalized & incidentally test positive for SARS-CoV-2 are NOT seen as COVID hospitalizations or deaths
This is a sharp contrast to the CDC’s stance during the pandemic🧵
This is a sharp contrast to the CDC’s stance during the pandemic🧵
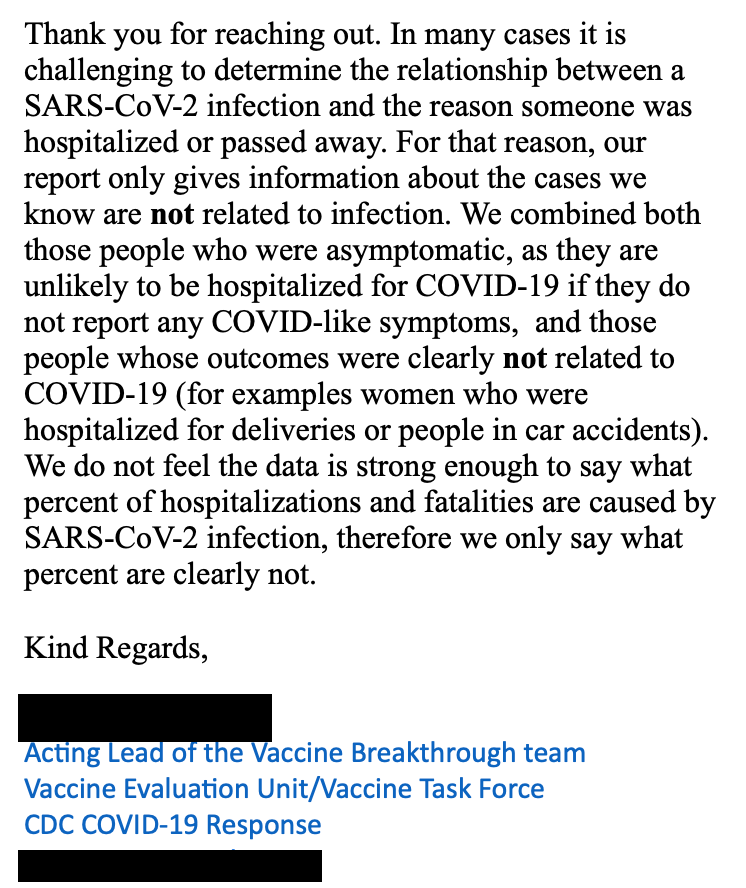
2/The email was a response to my inquiry re: data in the team's 5/28/21 report. I asked about the diff (if any) btw 2 categories of vaxed patients
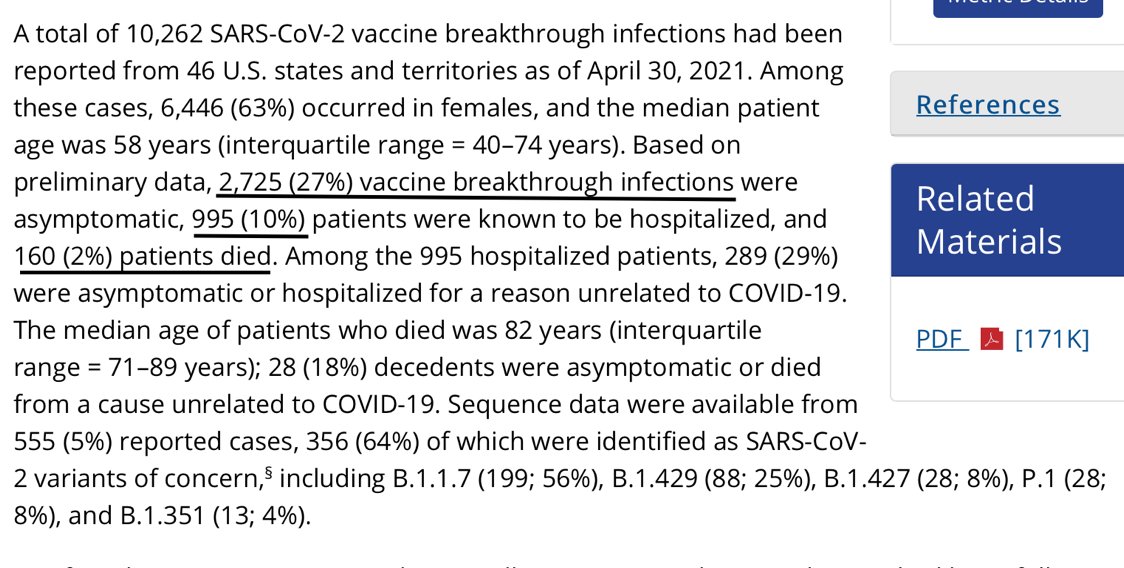
Researcher confirmed "asymp or hospitalized for a reason unrelated to COVID-19" are mutually exclusive cdc.gov/mmwr/volumes/7…
Researcher confirmed "asymp or hospitalized for a reason unrelated to COVID-19" are mutually exclusive cdc.gov/mmwr/volumes/7…
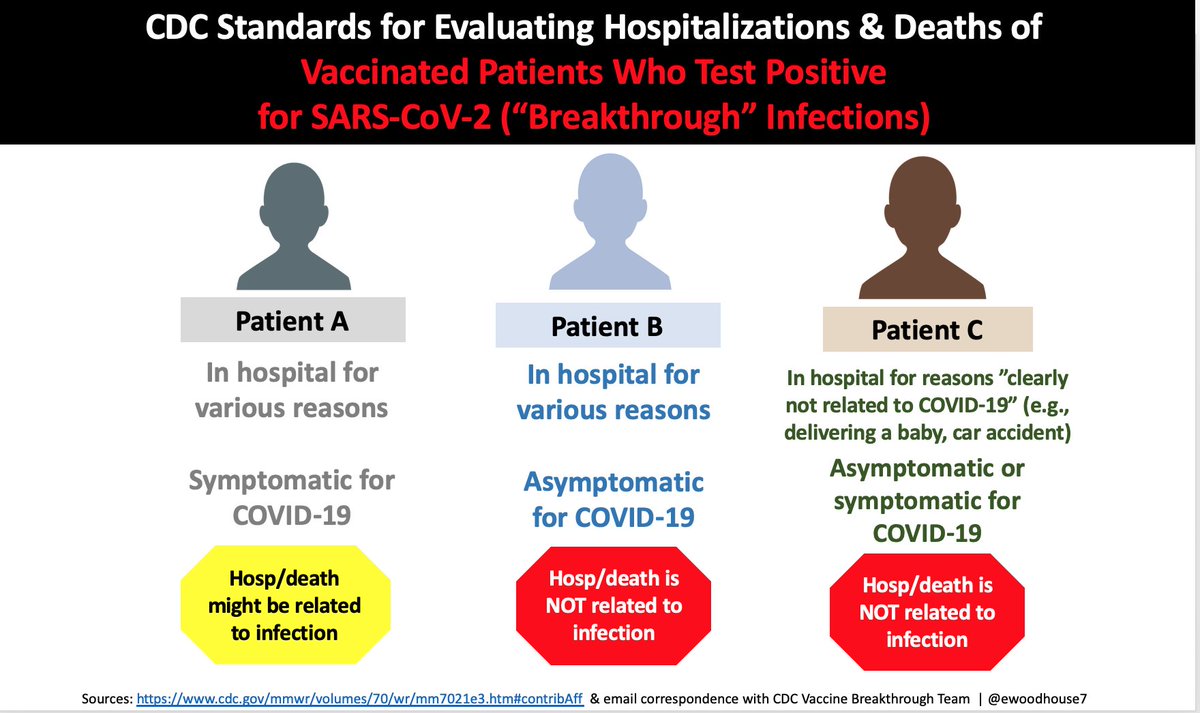
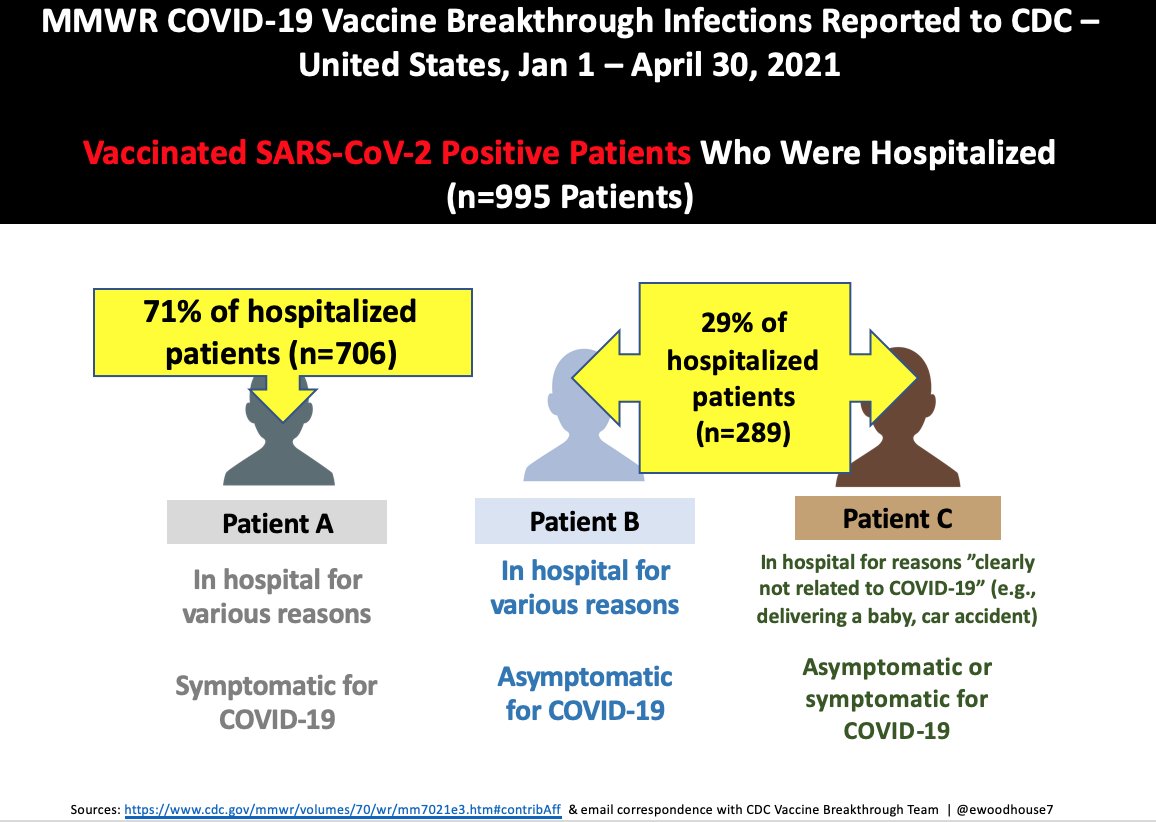
3/ Evaluating reported breakthru infections, the CDC team distinguishes 3 kinds of hosp patients. Per email, Patients B & C are "cases [they] know are not related to infection...whose outcomes were clearly NOT related to C19."
Patient A? Data "isn’t strong enough to say"
Patient A? Data "isn’t strong enough to say"
4/ Per the team's end of May report, nearly 30% of vaccinated hospitalized-for-some-reason patients tested positive for the virus.
Again, the lead researcher says these are "cases we know are not related to infection."
Again, the lead researcher says these are "cases we know are not related to infection."
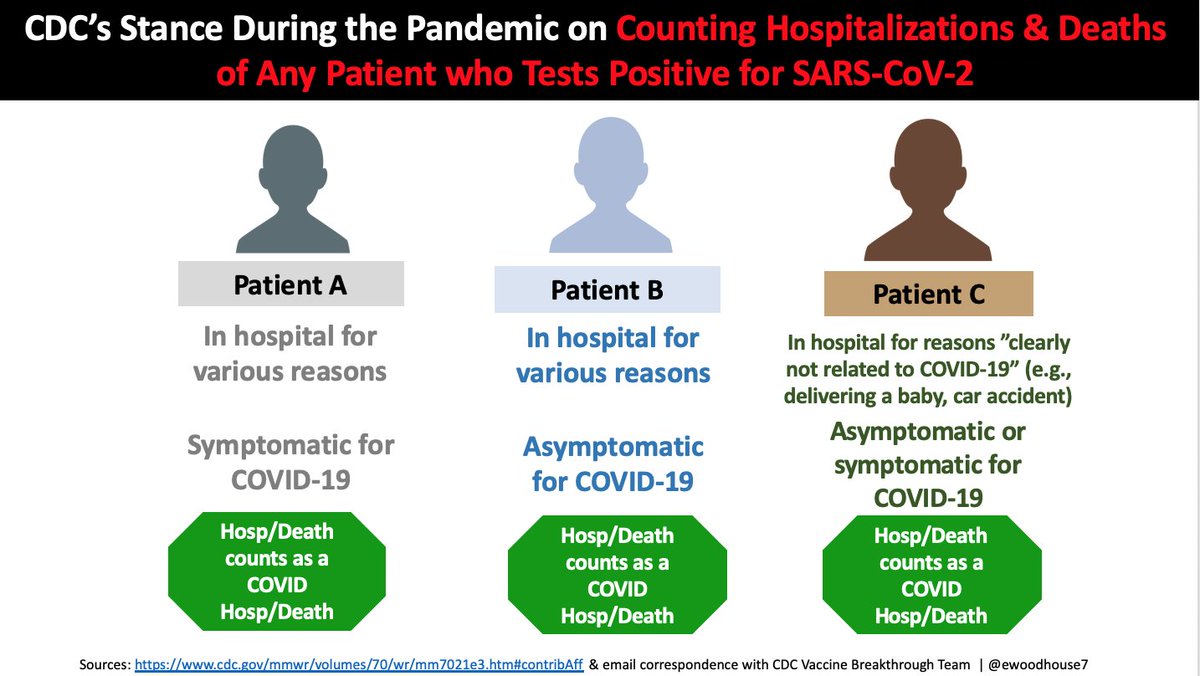
5/This is a departure from the CDC's implicit counting standards that have been applied throughout the pandemic
All three "positive patient types" are included in local, state, & national data -- even tho there's no reason Patient B or C should be in case, hosp, or death numbers
All three "positive patient types" are included in local, state, & national data -- even tho there's no reason Patient B or C should be in case, hosp, or death numbers
6/ To be clear, I agree with the approach in the left image, as a starting point for reporting ALL data - not just breakthrough infections.
What would our national numbers look like if it were applied?
Hint: very different
What would our national numbers look like if it were applied?
Hint: very different


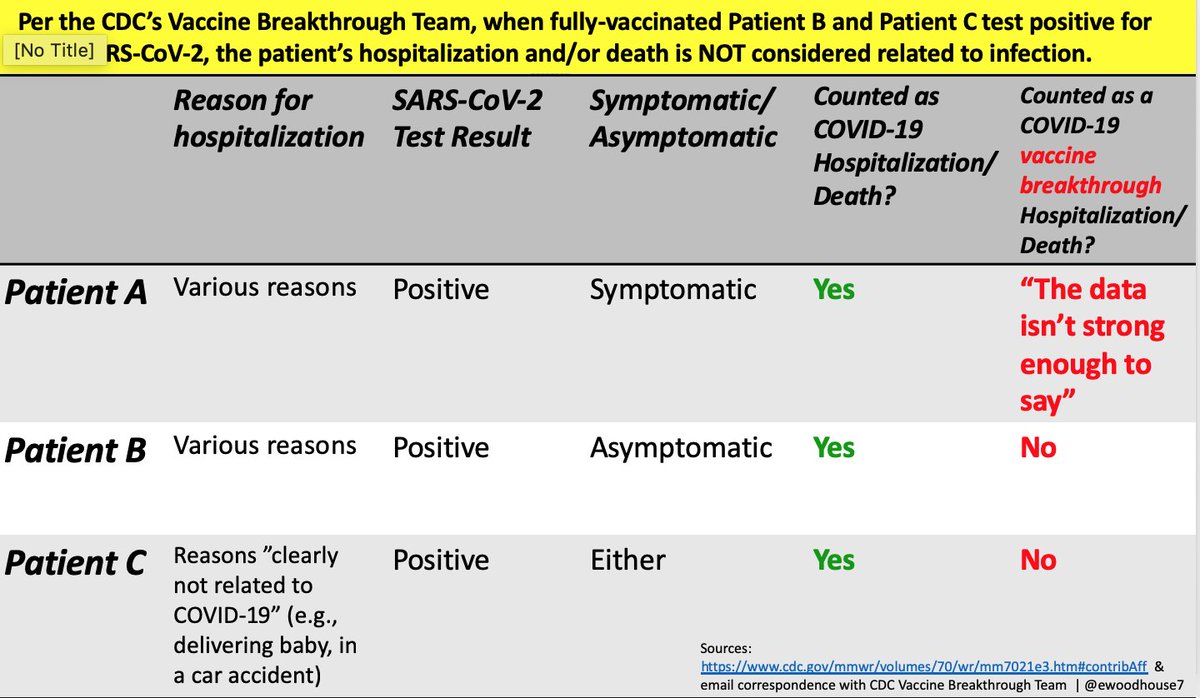
7/ Here's a table view of the same information.
Again, there's no earthly reason for the differential standards.
Again, there's no earthly reason for the differential standards.
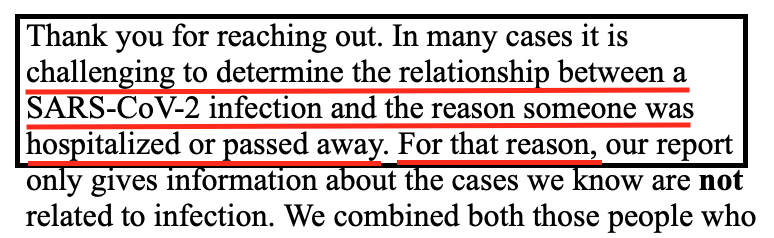
8/ In many ways, the first sentence in the email is the most 😳
Quite an admission from the agency that has liberally defined COVID cases, hospitalizations, & deaths for over a year - to the detriment of the economy, mental health, & societal fabric, among other things
Quite an admission from the agency that has liberally defined COVID cases, hospitalizations, & deaths for over a year - to the detriment of the economy, mental health, & societal fabric, among other things
9/ I don’t wish COVID were smallpox, but the truth is, many deadly pathogens have clear-cut, telltale signs that leave little doubt about cause.
By contrast, for this virus, we have the "any death within x number of days of a positive test" definition.
Sloppy, at best.
By contrast, for this virus, we have the "any death within x number of days of a positive test" definition.
Sloppy, at best.
• • •
Missing some Tweet in this thread? You can try to
force a refresh