ICMR-NIV study on P.2, the variant originally found in Brazil since ~April 2020 (WHO). Also called B.1.1.28.2 or zeta, it is now being rapidly replaced by P.1 in Brazil.
ICMR/NIV observed its effects on hamsters in comparison with P.1.
See thread
1/13
biorxiv.org/content/10.110…
ICMR/NIV observed its effects on hamsters in comparison with P.1.
See thread
1/13
biorxiv.org/content/10.110…
Presenting some context first. This variant P.2 was only seen in 2 samples so far in India; from asymptomatic travelers who arrived from Brazil and UK.
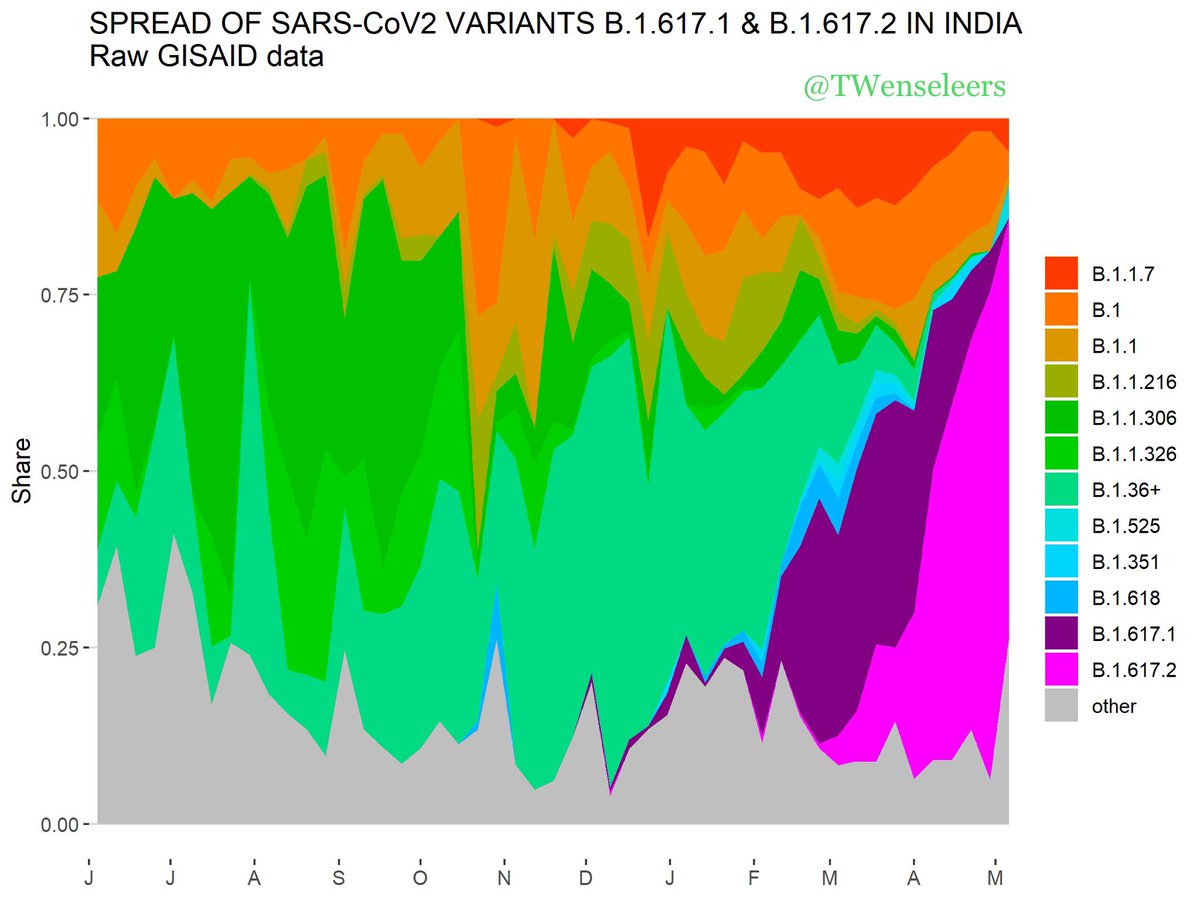
In Brazil, it is also being phased out by P.1 (deeper colour in recent weeks of 2021, genomic data from Manaus, Brazil).
2/13
In Brazil, it is also being phased out by P.1 (deeper colour in recent weeks of 2021, genomic data from Manaus, Brazil).
2/13


Study from Brazil showing how P.2 is being phased out by P.1. The latter variant has the N501Y mutation in addition to E484K, among several others.
3/13
virological.org/t/increasing-f…
3/13
virological.org/t/increasing-f…
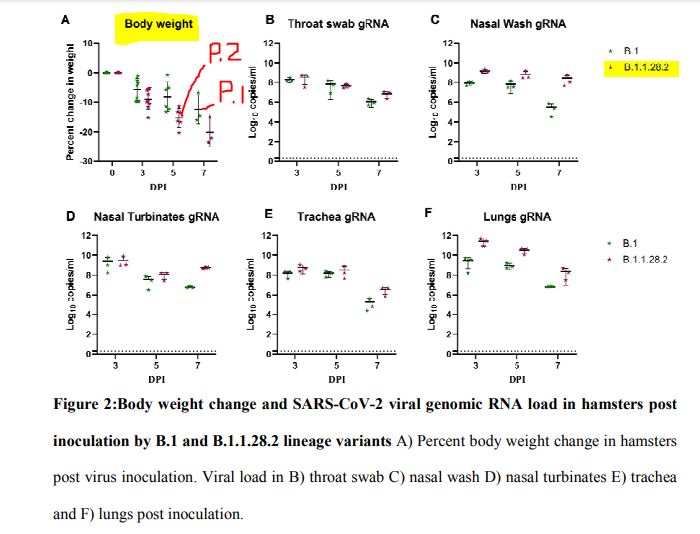
The ICMR/NIV study on hamsters showed that compared to P.1, the animals appeared to develop more severe lung disease.
9 hamsters each were infected with P.1 & P.2. The clinical parameters suggested P.2 was more severe, but the changes were not statistically significant.
4/13
9 hamsters each were infected with P.1 & P.2. The clinical parameters suggested P.2 was more severe, but the changes were not statistically significant.
4/13

An earlier study by ICMR/NIV had shown that only minimal loss of neutralisation occurred with this variant against covaxin (1.9 fold) & from sera (1.09) from natural infection. This reduction is not huge in comparison with other studies on variants.
5/13
vaccine.icmr.org.in/images/pdf/Bra…
5/13
vaccine.icmr.org.in/images/pdf/Bra…
This earlier ICMR study (see thread) implies that the variant P.2, in spite of the mutation E484K (shared with several other variants including P.1 & B.1.351) might not have the firepower needed to escape protection by vaccines, though it has been implied in reinfection.
6/13
6/13
P.2 has been implicated in two cases of reinfection in Brazil, see the paper attached and the pre-print below
7/13
thelancet.com/article/S0140-…
7/13
thelancet.com/article/S0140-…
Reinfection of a 45 year healthcare executive during October 2020 in Brazil, suggests P.2 variant was involved.
8/13
preprints.org/manuscript/202…
8/13
preprints.org/manuscript/202…
In Kerala, India @bani_jolly @vinodscaria et al studied breakthrough infections in 6 fully vaccinated healthcare workers (Covishield)
4/6 cases were from B.1.1.7.
None of these were severe.
One case had E484K; N501Y was noted in four (B.1.1.7).
9/13
pubmed.ncbi.nlm.nih.gov/34044037/
4/6 cases were from B.1.1.7.
None of these were severe.
One case had E484K; N501Y was noted in four (B.1.1.7).
9/13
pubmed.ncbi.nlm.nih.gov/34044037/

The Kerala breakthrough infections (see thread) occurred mostly in March & 1st week of April, that was before B.1.617.2 replaced B.1.1.7 as the dominant variant. This explains the variance of these findings with Delhi, where 48% breakthrough infections were B.1.617.2
10/13
10/13
48% of breakthrough infections that occurred in 69 (2.6%) of 3235 vaccinated healthcare workers in Delhi Apollo hospital were from B.1.617.2 (Delta) variant. Covishield was used here, 51 of 69 had received both doses.
11/13
thehindu.com/news/cities/De…
11/13
thehindu.com/news/cities/De…
It is however important to keep track of variants as they arrive / emerge, and study their ability to cause disease, speed of spread, & capability to escape protection from vaccines.
These studies from ICMR/NIV are proof that such diligence exists, and this is reassuring.
12/13
These studies from ICMR/NIV are proof that such diligence exists, and this is reassuring.
12/13
The @ThePrintIndia writes about how P.2 variant was discovered in India. See detailed thread above.
13/13
theprint.in/science/icmr-s…
13/13
theprint.in/science/icmr-s…
• • •
Missing some Tweet in this thread? You can try to
force a refresh