So Monica Gandhi and Kyle Hunter made a few mistakes in their piece on kids and the pandemic, specifically in suicidology. With additional context, a lot of their points about MH and the pandemic specifically melt away. I'll enumerate them.
/1
/1
First, she claims that there was an increase of 24% child suicides in california (by rate it's 24-27%) in 2020. She points to data for 2019, 2018, 2017 to show that this is an anomaly.
/2
/2

In fact, this is true. However, some additional context (or, had she consulted a suicidologist) sort of undermine this argument. The suicide rate has increased by 24% or more 4 times prior to 2020 in the past 20 years, and does so with a regular frequency.
excel data, CDC
/3
excel data, CDC
/3

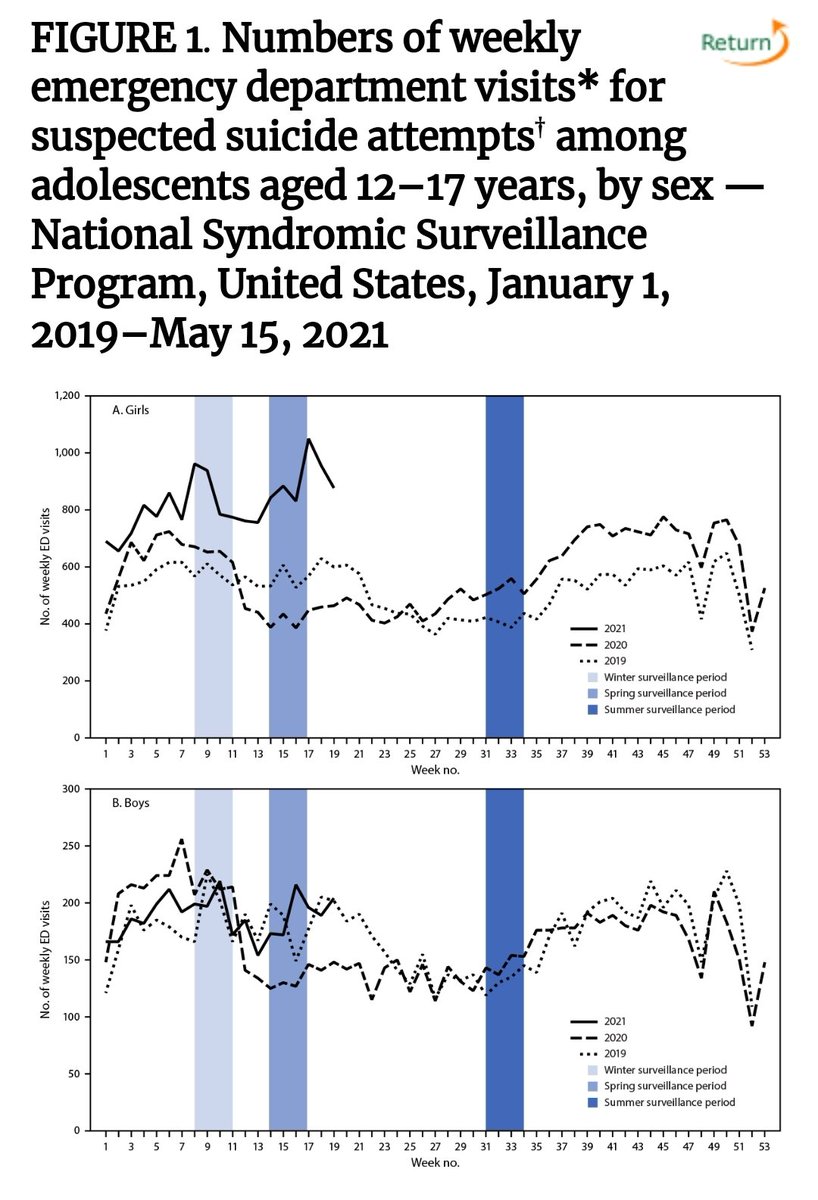
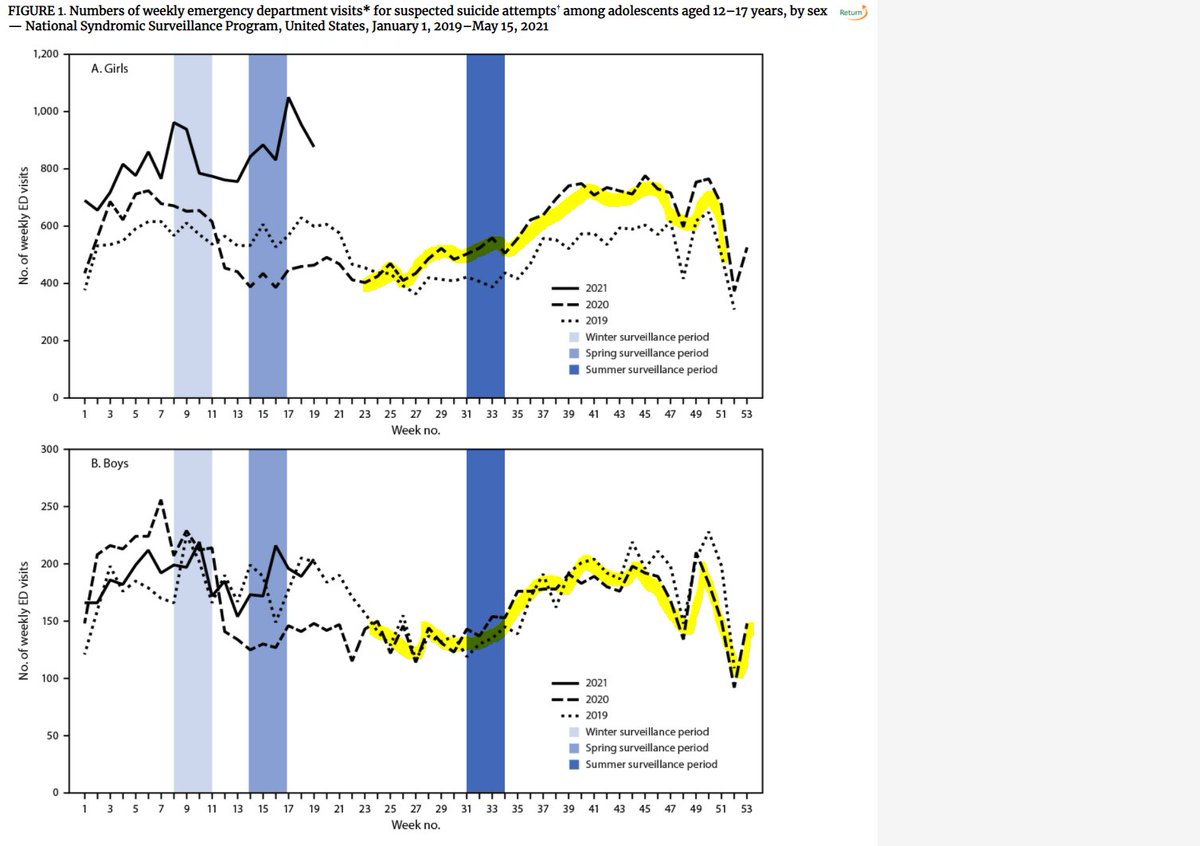
Next, she makes the point that the CDC just showed a 50% increase among (mainly) girls during the pandemic.
Significant editing is required.
/4
Significant editing is required.
/4

The CDC data has issues (discussed before, but it's data & it DOES show increase in distress in girls for sure. But only girls. not "mainly" girls. For boys, there was no difference. And it was not "during the pandemic."
/5
/5
For the first portion of the pandemic, rates of ER presentations were lower for both girls and boys, and country wide, almost every school was closed.
/6
/6

For the 2nd portion, there was a split in ER presentations b/w girls & boys, with boys returning to baseline & girls up by about 10%. This is during the end of school yr, the summer, and new school year, where school attendance really depended on state rules &conditions.
/7
/7
Certainly in Dr. Gandhi's jurisdiction, mostly closed. But across the US, there was a lot of variance on whether or not kids attended schools during this portion of the year.
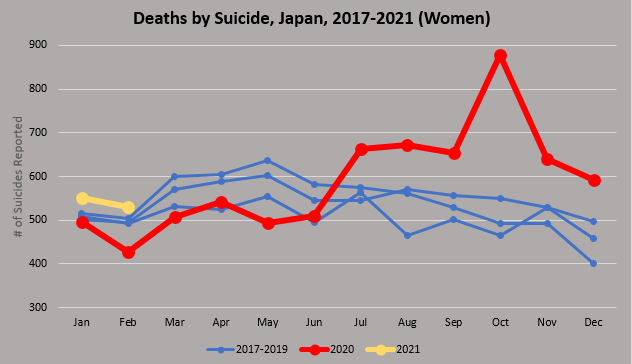
In my jurisdiction, BC Canada, schools have been open since September. Our SA/SI pattern was similar.
/8
In my jurisdiction, BC Canada, schools have been open since September. Our SA/SI pattern was similar.
/8
In the new year (2021+), we see this huge takeoff of girls and ER presentations, but this is during weeks 8-18, where almost half of schools are open across the United states. Remember, this is national data, not California data. And for whatever reason, only girls, not boys.
/9
/9

So for this spike to be related to school closures, it has to explain:
a) why only girls and not boys (unless I missed the memo that boys were totally off the hook and didn't have to go)
b) why the rates are increasing the more that schools are opening
/10
a) why only girls and not boys (unless I missed the memo that boys were totally off the hook and didn't have to go)
b) why the rates are increasing the more that schools are opening
/10
I think it should be concerning to Dr. Gandhi, who has maintained quite the ... sure ideological position... if adding context to the data she provides completely changes the weight of it as evidence of school closures being to blame.
/11
/11
In my jurisdiction, Vancouver, schools have been open full time since September (Trust me, my timeline is full of angry parents kids and teachers about this!!). I see kids professionally who are attending schools. And we have seen almost identical patterns in suicide/MH.
/12
/12
Those that are blaming school closures for mental health distress numbers might do a thing or two and examine their own evidence.
/13
/13
(regarding this data, i made strait population copy from 2020. this being a census year, it's difficult to know what happened with subset populations. the results do not change if the trend continues (27% increase) or reverses (24% increase)
I would also like to say that I believe in the principle of charity. I think the main reason this group of UCSF physicians are so convinced its school closures is because..well.. in their jurisdiction, schools are closed.
I don't think its malfeasance or incompetence. Just bias.
I don't think its malfeasance or incompetence. Just bias.
• • •
Missing some Tweet in this thread? You can try to
force a refresh