Short Tweetorial from my talk on Membranous Nephropathy: 2021 Update: #glomerular disease
1. Three types of Membranous- Primary, Secondary and Allo-immune
1. Three types of Membranous- Primary, Secondary and Allo-immune

2. Causes of secondary MN: Cancers, Drugs, Infections and autoimmune disease( like any other disease).
3. Class switching happens: be-aware

4. A positive anti-PLA2R antibody test is “virtually” diagnostic of a lesion of MN (but may not always be able to reliably distinguish primary and secondary forms)




6) Pathophysiology of MN

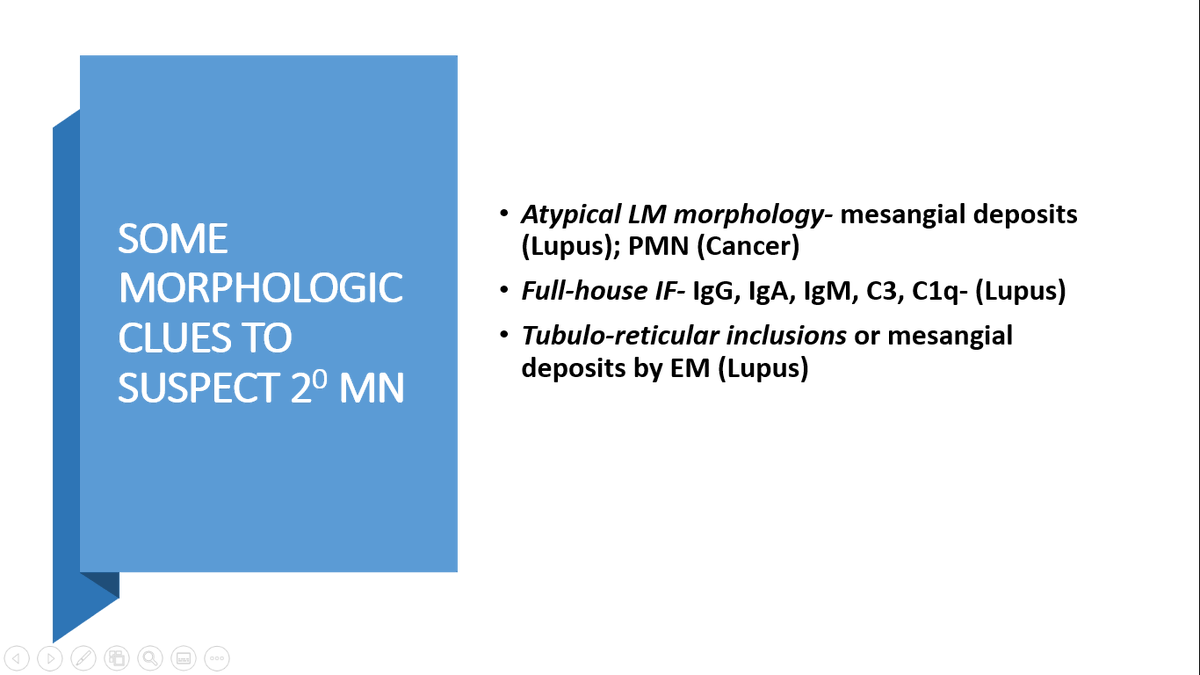
7) Pathophysiology of Secondary MN


8) Prognosis is unfavorable if Black race, age > 65 yr, Male, p/crt >8gm/dl >6mo, High BP/low GFR/ low Palb, Severe IFTA/FSGS, High aPLA2R ab titer, No remission with initial treatment
9) The role of PLA2R has evolved from just being diagnostic to prognostic and even following the disease


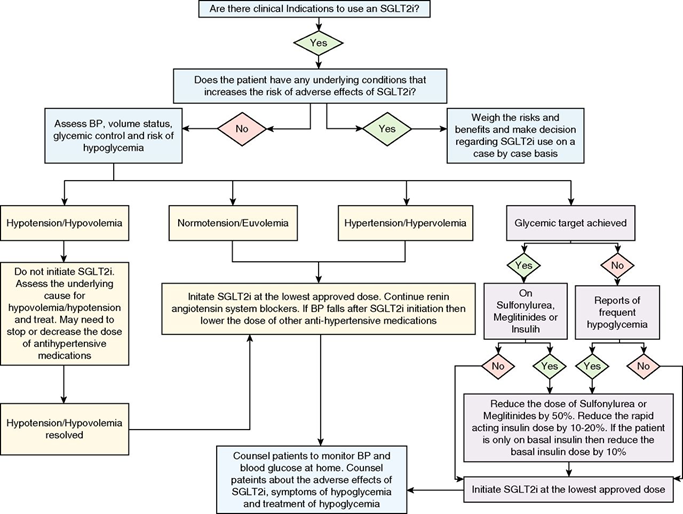
10). When do we do kidney biopsies and when do we do anticoagulation? @goKDIGO


11) Treatment summary:
Alkylating agents – best proven treatment
CNI- higher relapses
MENTOR trial( Rituximab vs CNI) and STARMEN study( tacrolimus and rituximab vs modified Ponticelli regimen) and Ri-CYCLO( Modified Ponticelli vs rituximab)
Alkylating agents – best proven treatment
CNI- higher relapses
MENTOR trial( Rituximab vs CNI) and STARMEN study( tacrolimus and rituximab vs modified Ponticelli regimen) and Ri-CYCLO( Modified Ponticelli vs rituximab)
12) Evidence of Treatment
Steroids alone- Ineffective ( 1A)
Alkylating agents + Steroids- Effective for CR/PR and for preventing ESRD (1A)
Rituximab- Appears highly effective in RCT studies (1A)
Calcineurin inhibitors ± Steroids (CsA/Tac)Effective for PR; High relapse rate
Steroids alone- Ineffective ( 1A)
Alkylating agents + Steroids- Effective for CR/PR and for preventing ESRD (1A)
Rituximab- Appears highly effective in RCT studies (1A)
Calcineurin inhibitors ± Steroids (CsA/Tac)Effective for PR; High relapse rate
13)Azathioprine + Steroids- Ineffective
Mycophenolate mofetil (MMF)- data is poor
Natural ACTH- No RCT, no long-term studies. Relapse rate uncertain
Sirolimus- limited data- not recommended
Mycophenolate mofetil (MMF)- data is poor
Natural ACTH- No RCT, no long-term studies. Relapse rate uncertain
Sirolimus- limited data- not recommended


16) MENTOR- Ritux vs CNI nejm.org/doi/full/10.10…
1. RTX non inferior to CNI at 12 months
2. RTX superior at 24 months
1. RTX non inferior to CNI at 12 months
2. RTX superior at 24 months


17) Tacro_RTX combo vs Cyclical therapy( classic)
STARMEN TRIAL kidney-international.org/article/S0085-…
STARMEN TRIAL kidney-international.org/article/S0085-…

18) Ri-CYCLO trial- Cyclical vs Rituximab

19) what we have learned:
OLD IS GOLD( cyclo steroids cyclical therapy works and side effect profile not that bad as we thought)
PATIENT IS VIRTUE( give rituximab time to work)
OLD IS GOLD( cyclo steroids cyclical therapy works and side effect profile not that bad as we thought)
PATIENT IS VIRTUE( give rituximab time to work)









Interesting combo treatment option ajkd.org/article/S0272-… Combination of Rituximab, Low-dose Cyclophosphamide, and Prednisone for Primary Membranous Nephropathy @AJKDonline
• • •
Missing some Tweet in this thread? You can try to
force a refresh