One of my favourite things to see - despite being nearly 80, this patient is producing alpha oscillations with amplitude commensurate with a much younger brain!
Suggested pre-GA from excellent general health, non-smoker and cognitively pin-sharp (crosswords, reading club etc!)
Suggested pre-GA from excellent general health, non-smoker and cognitively pin-sharp (crosswords, reading club etc!)

This is a TIVA TCI anaesthetic. Predictably, these patients will emerge very well from anaesthesia.
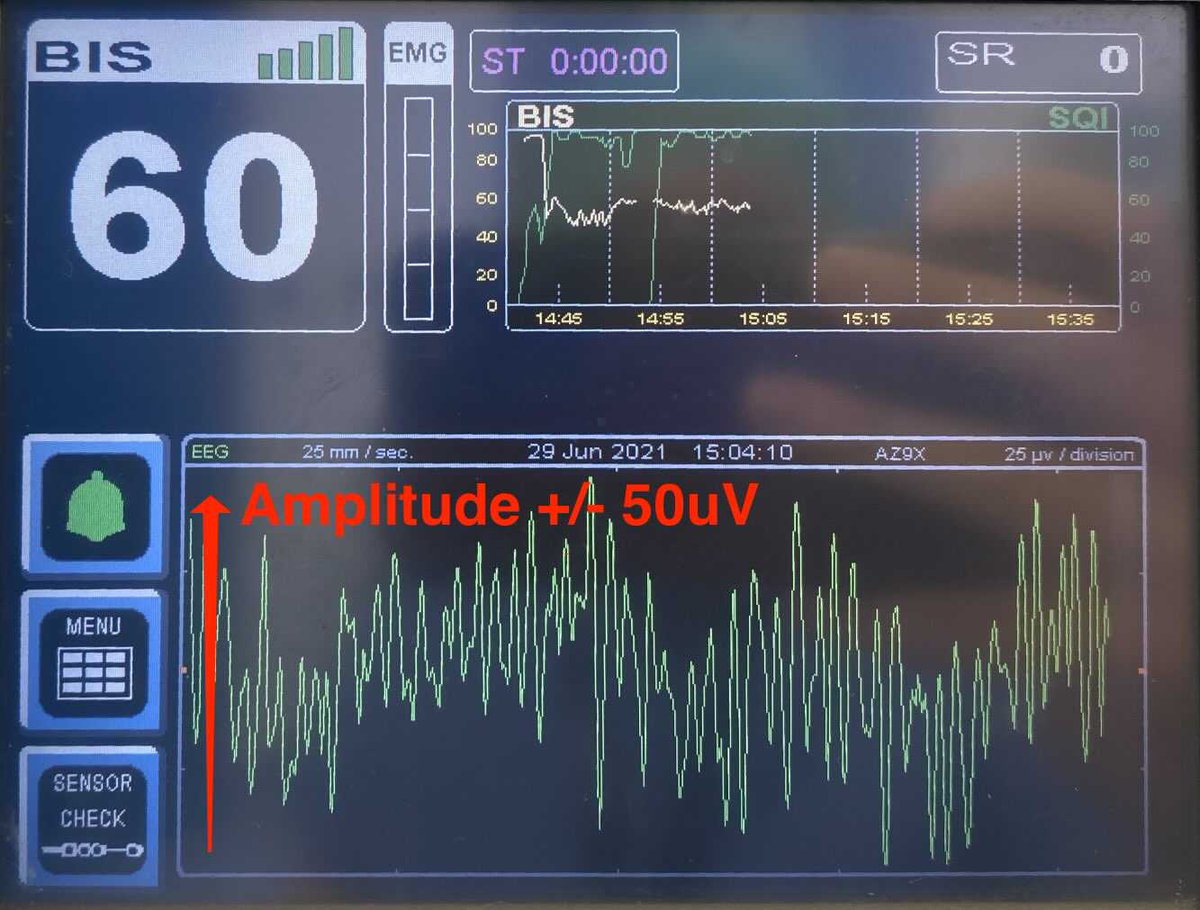
Although the BIS is simpler pEEG device than the Narcotrend or Sedline, one can still appreciate EEG features.
Although the BIS is simpler pEEG device than the Narcotrend or Sedline, one can still appreciate EEG features.
The X axis is time - this EEG epoch is 4.4 seconds long.
It’s worth remembering this.
(The device is actually uses 2 second epochs with a 1 second overlap in the algorithm but that doesn’t really matter unless you’re being really geeky, but sort of explains the 63 second SR)
It’s worth remembering this.
(The device is actually uses 2 second epochs with a 1 second overlap in the algorithm but that doesn’t really matter unless you’re being really geeky, but sort of explains the 63 second SR)

The Y axis is amplitude - this is fixed at +/-50uV.
Generally 50uV is pretty good for middle age, but older patients can have much lower amplitudes, and children much much higher!
-Amplitude peaks around 8 years old, then its down hill all the way.
[adjustable on Narco/Sedline]
Generally 50uV is pretty good for middle age, but older patients can have much lower amplitudes, and children much much higher!
-Amplitude peaks around 8 years old, then its down hill all the way.
[adjustable on Narco/Sedline]
Oddly BIS has a high pass filter at 2Hz - you must turn this OFF (3rd Menu screen) to see slow and delta oscillations!
These are Slow or Delta Waves* - 3 cycles / 4.4 seconds = 0.7Hz
These are Slow or Delta Waves* - 3 cycles / 4.4 seconds = 0.7Hz
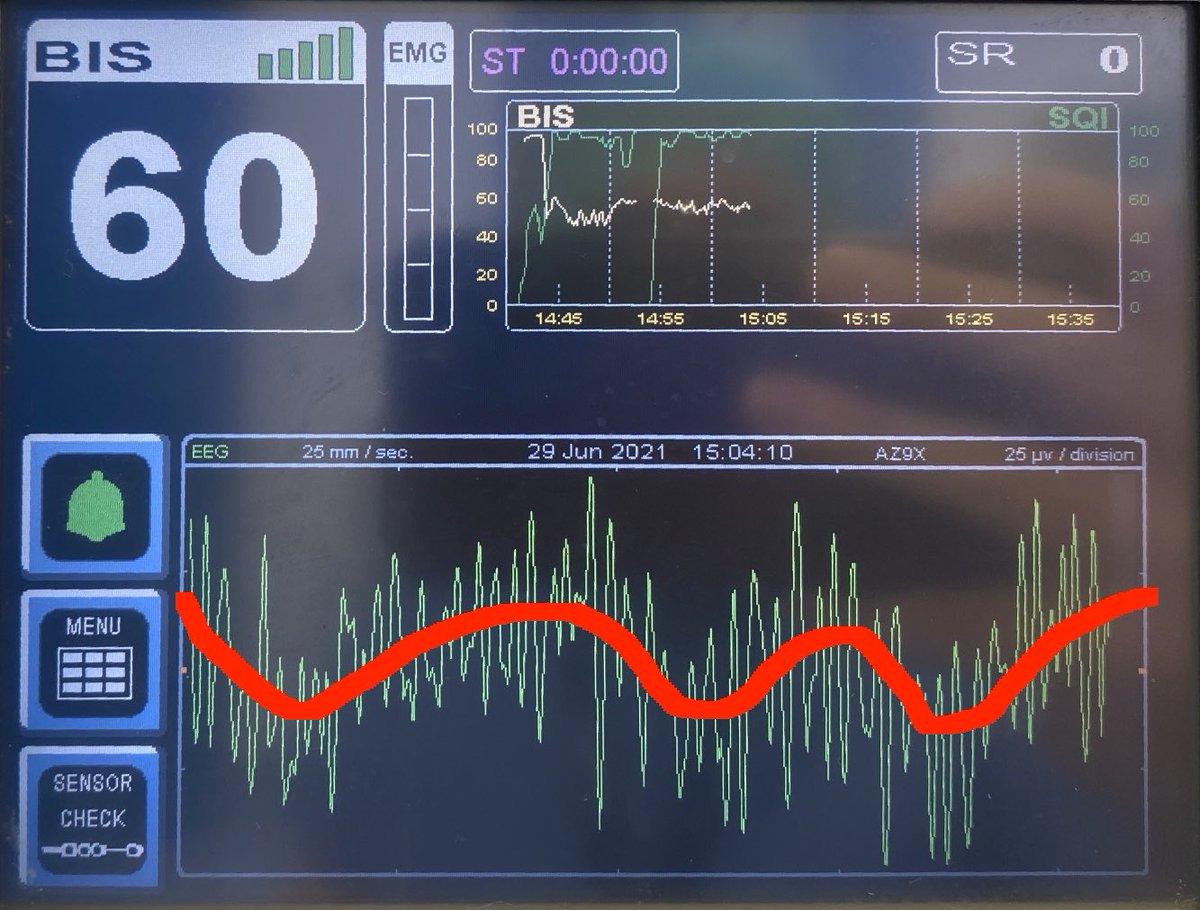
There are faster oscillations too!
52 or so.
52 / 4.4sec = 12Hz
These are alpha oscillations.
Typically with age, the alpha falls in both frequency AND power (slower and smaller).
Propofol produces this “alpha/delta” pattern on the EEG.
52 or so.
52 / 4.4sec = 12Hz
These are alpha oscillations.
Typically with age, the alpha falls in both frequency AND power (slower and smaller).
Propofol produces this “alpha/delta” pattern on the EEG.

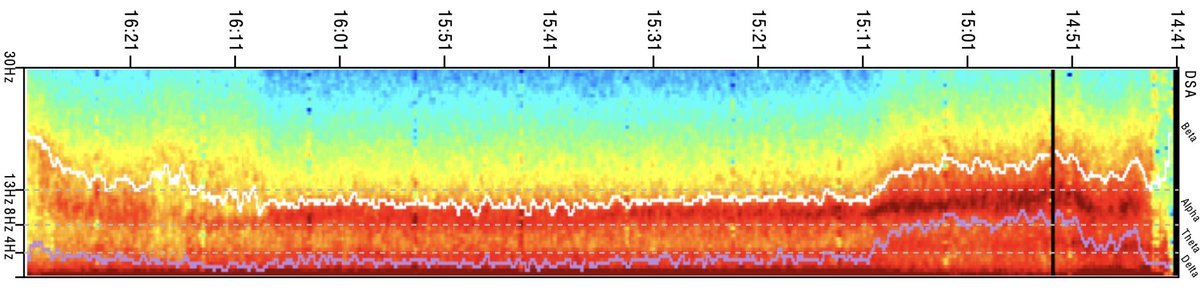
A more intuitive way to visualise the distribution of EEG oscillations over time is to use the Density Spectral Array.
I discussed the basics briefly here:
I discussed the basics briefly here:
Here’s the DSA for this patient, notice how “red” the alpha band is. Plenty of power here, that’s those great big oscillations!
Keen 👀 might notice a smidge of ketamine too 😎
[BIS has a VERY limited implementation of DSA vs Sedline and Narco;🤞🏼@Medtronic improve this!]
Keen 👀 might notice a smidge of ketamine too 😎
[BIS has a VERY limited implementation of DSA vs Sedline and Narco;🤞🏼@Medtronic improve this!]
Headaches with the @Medtronic BIS DSA are its the small size, lack of windowing and markers, and it prints backwards! Does anyone do QA before software releases?
(Lets not mention the SEF95 “quirk” ).
Do reach out if R&D want advice… 🤣
(Lets not mention the SEF95 “quirk” ).
Do reach out if R&D want advice… 🤣
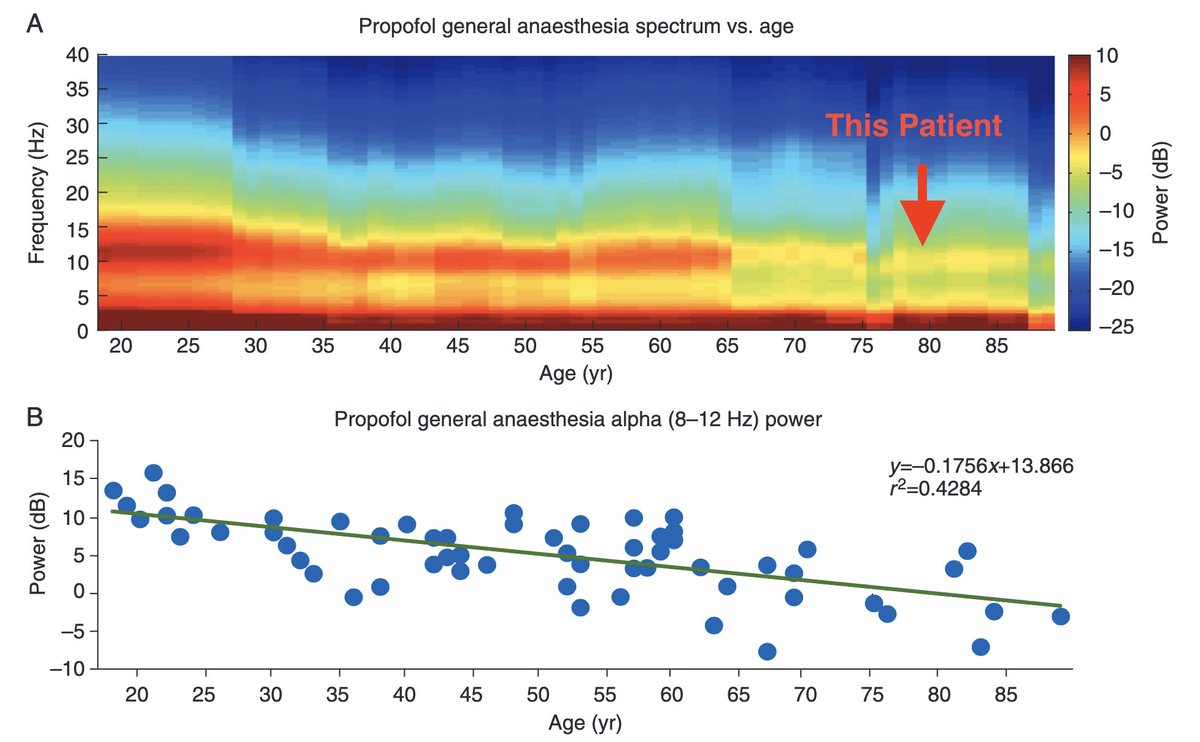
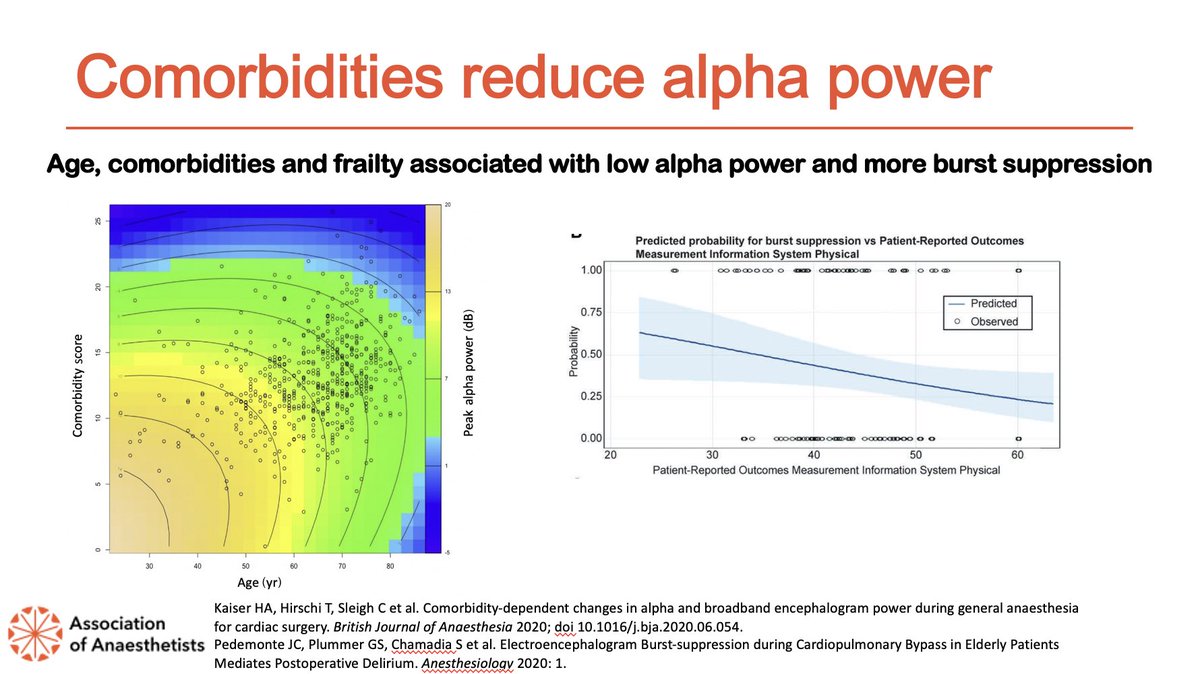
So what of age? Akeju, Purdon and Brown @MGHanesthesia and Schultz @narcotrend have written much on this.
Genuinely fascinating, and should be core @RCoANews Primary FRCA material.
Typically alpha power falls - noticeable from >65. But age isn’t just a biological construct!
Genuinely fascinating, and should be core @RCoANews Primary FRCA material.
Typically alpha power falls - noticeable from >65. But age isn’t just a biological construct!
Here’s a few more spectrograms - the reduction in alpha power is pretty apparent!
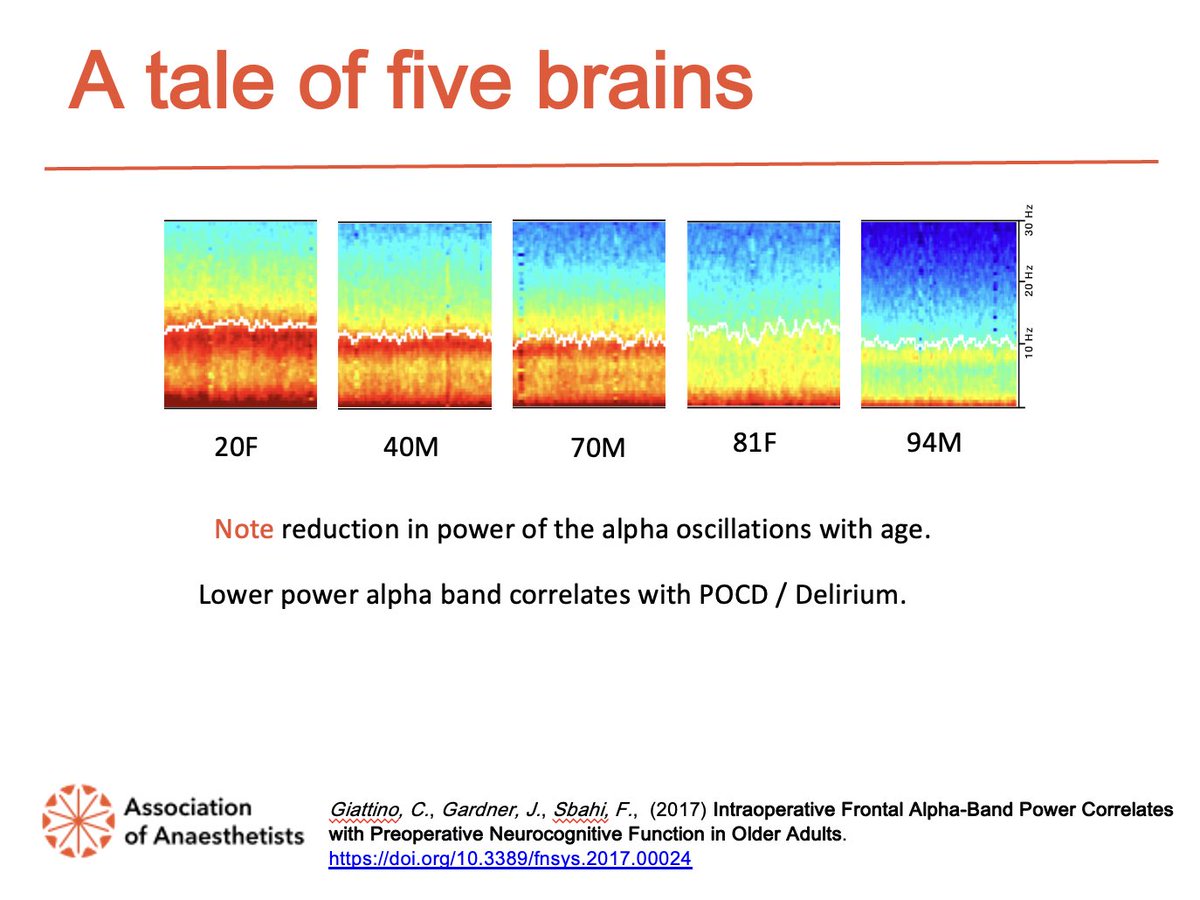
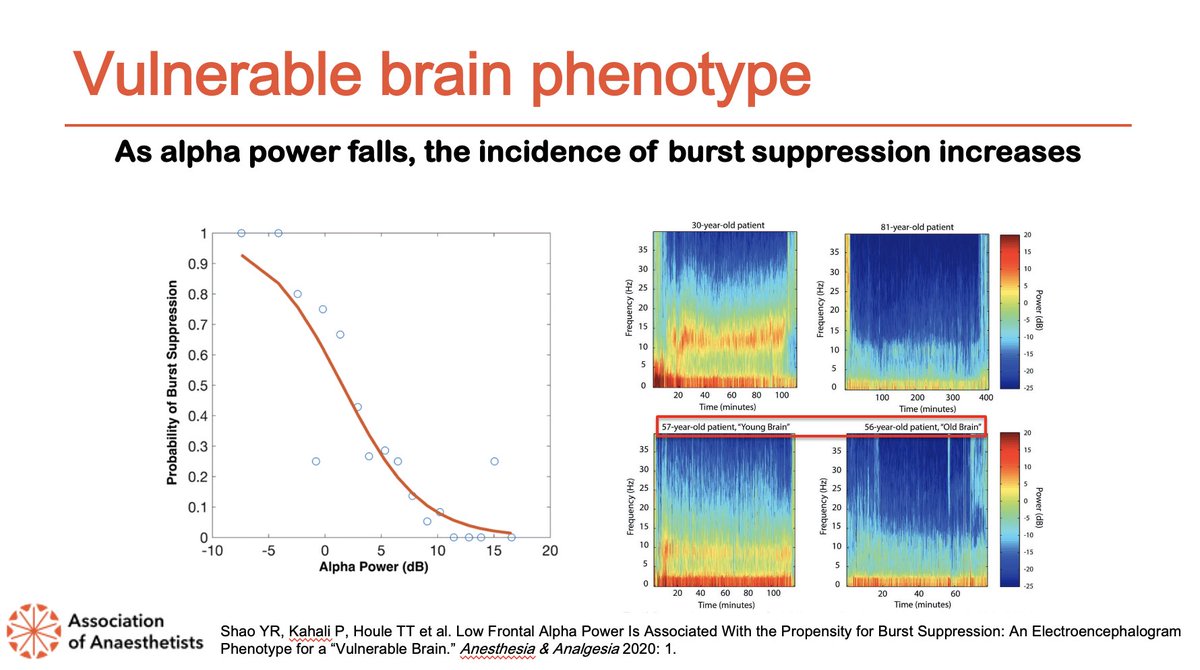
As alpha power falls, the incidence of burst suppression increases.
Burst suppression seems to be a marker of a “vulnerable brain”; time in burst suppression is related to post operative delirium.
BIS index isn’t tightly coupled to the suppression ratio - keep an eye on the SR!
Burst suppression seems to be a marker of a “vulnerable brain”; time in burst suppression is related to post operative delirium.
BIS index isn’t tightly coupled to the suppression ratio - keep an eye on the SR!
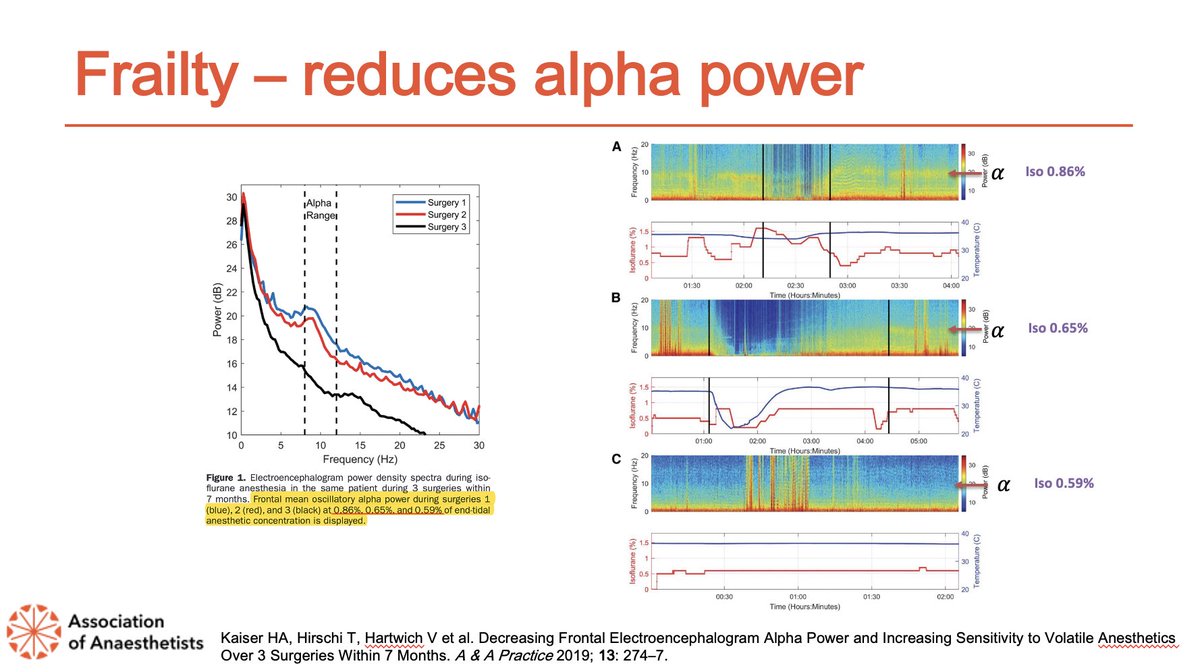
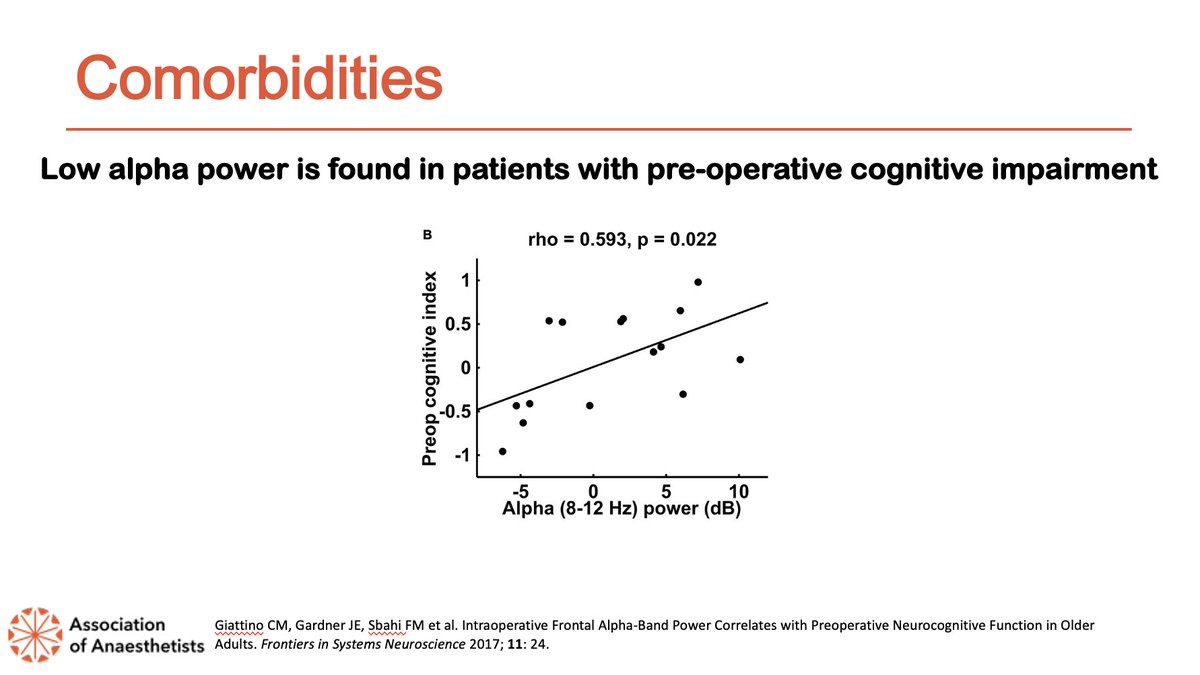
Frailty, co-morbidities and cognitive impairment also reduce alpha power.
Vascular patients seem to have the perfect storm for vulnerable brains.
Physical and mental exercise, and not smoking might be good for brain health.
Vascular patients seem to have the perfect storm for vulnerable brains.
Physical and mental exercise, and not smoking might be good for brain health.
This is one of my favourite quotes.
Anaesthesia is a “brain stress test”.
“If you don’t use intra-operative EEG you’ll never see this information”
Anaesthesia is a “brain stress test”.
“If you don’t use intra-operative EEG you’ll never see this information”
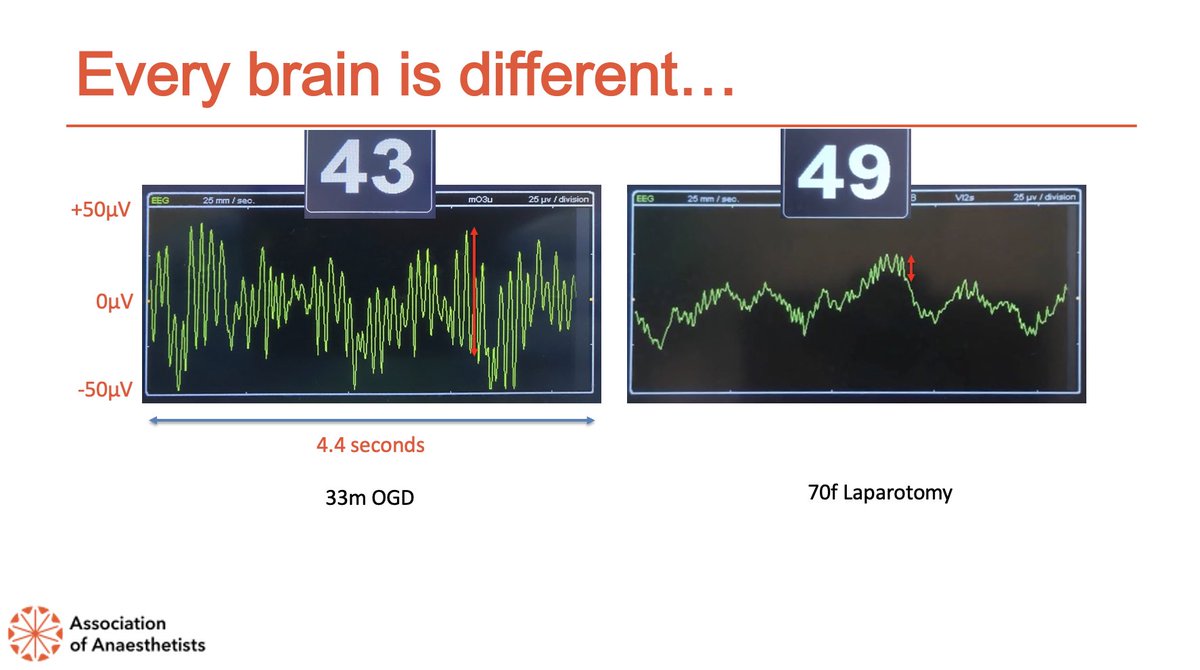
So what would a more typical “old” brain look like?
See below, our patient looks more like the young brain on the left!
See below, our patient looks more like the young brain on the left!
“60! Are you mad?!”
There’s more to pEEG than numbers; reassuring alpha/delta EEG & DSA, no noiceptive responses with clinically appropriate drug delivery is more valuable!
BIS over-reads by 2 ABU’s per decade (>40) at 1 aaMAC 🤔
There’s more to pEEG than numbers; reassuring alpha/delta EEG & DSA, no noiceptive responses with clinically appropriate drug delivery is more valuable!
BIS over-reads by 2 ABU’s per decade (>40) at 1 aaMAC 🤔

There’s fantastic pEEG CPD here:
icetap.org
eegforanesthesia.iars.org
The QR code below should link to my “essential” pEEG reading, YouTube and podcast list!
icetap.org
eegforanesthesia.iars.org
The QR code below should link to my “essential” pEEG reading, YouTube and podcast list!

@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh