
#TumorBoardTuesday
CASE PRESENTATION
65 year old man presents with pain in the right upper quadrant of his abdomen and weight loss. (1/n)
CASE PRESENTATION
65 year old man presents with pain in the right upper quadrant of his abdomen and weight loss. (1/n)

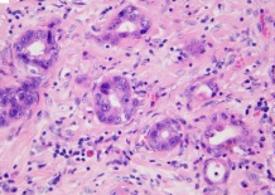
Core needle biopsy of the liver mass shows adenocarcinoma. Immunohistochemical (IHC) testing was positive for CK7 and CK20. IHC was negative for TTF1 and HepPar1.
Photo taken from a very nice review from @VijgenSandrine ncbi.nlm.nih.gov/pmc/articles/P… #TumorBoardTuesday (2/n)
Photo taken from a very nice review from @VijgenSandrine ncbi.nlm.nih.gov/pmc/articles/P… #TumorBoardTuesday (2/n)
Imaging studies reveal a dominant liver mass & satellite liver lesions. The patient also has peritoneal and lung metastases.
Labs showed no abnormalities other than CA 19-9 of 15,000 and CEA of 100.
The patient is diagnosed with metastatic intrahepatic cholangiocarcinoma. (3/n
Labs showed no abnormalities other than CA 19-9 of 15,000 and CEA of 100.
The patient is diagnosed with metastatic intrahepatic cholangiocarcinoma. (3/n
Despite the pain, the patient is still working and doing his normal activities (ECOG performance status = 1)
He reports no other medical problems or family history of cancer.
#TumorBoardTuesday (4/n)
He reports no other medical problems or family history of cancer.
#TumorBoardTuesday (4/n)
Poll: What would you use for the first-line of chemotherapy?
The patient was treated with first-line Gemcitabine/Cisplatin based on data from the ABC-02 trial.
nejm.org/doi/full/10.10…
#TumorBoardTuesday (5/n)
nejm.org/doi/full/10.10…
#TumorBoardTuesday (5/n)
We are eagerly awaiting the results of the phase 3 SWOG 1815 trial evaluating gemcitabine/cisplatin/nab-paclitaxel. The phase 2 trial of this combination was promising. @rachnatshroff @JavleMilind @GIcancerDoc @kmody29
ja.ma/3k6zMN0 via @JAMAOnc part of @JAMANetwork 6/n
ja.ma/3k6zMN0 via @JAMAOnc part of @JAMANetwork 6/n
POLL: Would you order next generation sequencing in this patient while they are getting first-line chemotherapy?
Genomic studies have revealed that about 45% of intrahepatic cholangiocarcinoma (IHCC) patients have tumors that harbor an actionable genomic alteration. This table shows the genomic alterations seen in our series at @DanaFarberNews.
#TumorBoardTuesday (7/n)
#TumorBoardTuesday (7/n)

BACK TO THE PATIENT
While receiving first-line gemcitabine/cisplatin, next generation sequencing (NGS) testing on the patient’s liver biopsy was ordered.
#TumorBoardTuesday (8/n)
While receiving first-line gemcitabine/cisplatin, next generation sequencing (NGS) testing on the patient’s liver biopsy was ordered.
#TumorBoardTuesday (8/n)
NGS revealed that the cancer is microsatellite stable with a TMB of 6.
His cancer had the following alterations:
FGFR2 p.H167_N173del
Two copy deletion of CDKN2A/B
#TumorBoardTuesday (9/n)
His cancer had the following alterations:
FGFR2 p.H167_N173del
Two copy deletion of CDKN2A/B
#TumorBoardTuesday (9/n)
The patient’s cancer progresses on gemcitabine/cisplatin after 7 months of therapy. While more fatigued, the patient still has good organ function and performance status.
#TumorBoardTuesday (10/n)
#TumorBoardTuesday (10/n)
POLL: What second-line therapy do you recommend?
The pt decides to proceed with an FGFRi and is treated with off-label pemigatinib. Potential toxicities include hyperphosphatemia, nail changes, retinal toxicity, and cutaneous toxicity. See previous #tumorboardtuesday by @ebbenjohnathan for discussion on FGFRi toxicities.(11/n)
FGFR2 translocations are present in 15% of intrahepatic cholangiocarcinomas. A major milestone was the FDA approval of FGFR inhibitors in cholangiocarcinoma. The first FGFRi approved was pemigatinib. @gaboualfa @miteshborad @doccatenacci thelancet.com/journals/lanon…
(12/n)
(12/n)
A few weeks ago, a 2nd FGFR inhibitor, Infigratinib (BGJ398), was FDA approved for patients with cholangiocarcinoma harboring an FGFR2 translocation. @JavleMilind @rachnatshroff @MiteshBorad @DrElkhoueiry @GABOUALFA @GIcancerDoc pubmed.ncbi.nlm.nih.gov/29182496/
#TumorBoardTuesday (13/n)
#TumorBoardTuesday (13/n)
The success of FGFR inhibition in FGFR2 translocated cholangiocarcinoma raises the question of whether there are other FGFR2 genomic alterations that predict sensitivity to FGFR inhibitors.
#TumorBoardTuesday (14/n)
#TumorBoardTuesday (14/n)
We observed several patients with FGFR2 extracellular domain in-frame deletions (INDELs) who had substantial responses to FGFR inhibitors. We see FGFR2 INDELs in about 2%-3% of intrahepatic cholangiocarcinoma patients.
cancerdiscovery.aacrjournals.org/content/early/…
#TumorBoardTuesday (15/n)
cancerdiscovery.aacrjournals.org/content/early/…
#TumorBoardTuesday (15/n)
To explain why we think FGFR2 extracellular domain in-frame deletions are sensitive to FGFR inhibitors, I first want to briefly review ways that FGFR2 can become activated.
#TumorBoardTuesday (16/n)
#TumorBoardTuesday (16/n)
The #FGFR2 receptor ordinarily becomes activated when its ligand, FGF, promotes its dimerization. FGFR2 translocations cause constitutive FGFR2 activation because the FGFR2 fusion partner has an intracellular dimerization domain. @li_fangda pubmed.ncbi.nlm.nih.gov/31899106/ (17/n)

In a very sad congenital abnormality, called #Craniosynostosis Syndrome, premature bone suture fusion occurs in infancy leading to craniofacial deformities. Genomic analysis revealed that these syndromes are typically caused by activating germline FGFR alterations. (18/n)
Extracellular FGFR2 alterations that cause #Craniosynostosis promote dimerization and activation of the FGFR2 receptor. These FGFR2 alterations can increase the affinity of FGFR2 for FGF or, by eliminating cysteine residues, lead to the formation of aberrant disulfide bonds(19/n
Like the #FGFR2 alterations that cause Craniosynostosis, FGFR2 extracellular INDELs activate FGFR2. In silico modeling predicts that the INDELs promote receptor dimerization. In cell lines, FGFR2 p.H167_N173del causes oncogenic transformation that is sensitive to FGFRi. (20/n)

The important clinical point is that we are finding #FGFR2 extracellular in-frame deletions in 2-3% of intrahepatic cholangiocarcinoma patents. SO PLEASE LOOK FOR THEM!!!! Interestingly, we also found them in #breastcancer, #uterinecancer, and #lungcancer
#TumorBoardTuesday (21/n
#TumorBoardTuesday (21/n

BACK TO THE PATIENT
The patient’s cancer responds well to pemigatinib. However, after 12 months the cancer develops acquired resistance. Molecular profiling of a repeat biopsy shows development of a new FGFR2 kinase domain mutation FGFR2 p.L618F
#TumorBoardTuesday (22/n)
The patient’s cancer responds well to pemigatinib. However, after 12 months the cancer develops acquired resistance. Molecular profiling of a repeat biopsy shows development of a new FGFR2 kinase domain mutation FGFR2 p.L618F
#TumorBoardTuesday (22/n)
Lipika Goyal and Nabeel Bardeesy demonstrated that the irreversible FGFR2 inhibitor futibatinib (TAS-120) can overcome acquired resistance caused by reversible FGFR inhibitors like pemigatinib and infigratinib.
cancerdiscovery.aacrjournals.org/content/9/8/10…
#TumorBoardTuesday (23/n)
cancerdiscovery.aacrjournals.org/content/9/8/10…
#TumorBoardTuesday (23/n)
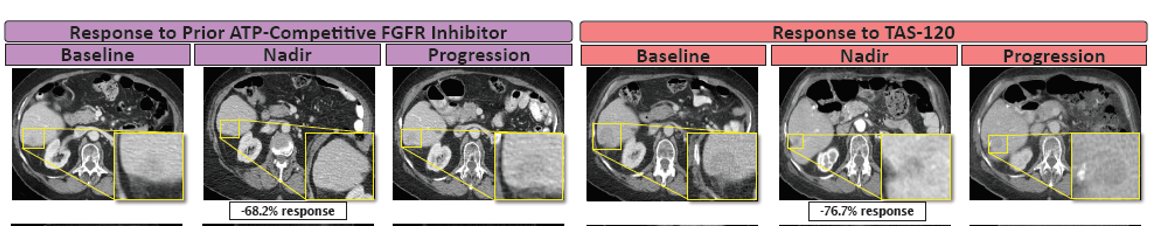
The patient’s cancer has an 11-month response to compassionate use futibatinib (TAS-120)!
Ultimately, the cancer develops acquired resistance and cell-free DNA shows development of NRAS and KRAS mutations.
#TumorBoardTuesday (24/n)
Ultimately, the cancer develops acquired resistance and cell-free DNA shows development of NRAS and KRAS mutations.
#TumorBoardTuesday (24/n)
Thanks everyone for this great discussion. I should mention that the patient discussed was fictional but based on the things we've learned from our cohort of INDEL patients (25/n).
• • •
Missing some Tweet in this thread? You can try to
force a refresh


