Next up Mats Wahlstrom on The Next Generation of Dialysis. Former CEO of Fresenius and Gambro. #AspenKidney
We are seeing a major investment in home therapies. Credits government initiatives. We are currently at 2% home hemo and 10% PD. #AspenKidney
He credits NextStage as putting home hemo back on the map. Small. Portable. Easy to use. Online dialysat4e production. Major driver of success: Capturing commercial payers! #AspenKidney
Fresenius bought NextStage for 2 billion dollars in 2019 #AspenKidney
Other options on the horizon:
Tablo by Outset Medical. Real time dialysate production
Quanta from the UK raised $245 million
CVS Kidney Care
#AspenKidney
Tablo by Outset Medical. Real time dialysate production
Quanta from the UK raised $245 million
CVS Kidney Care
#AspenKidney
The major investment in PD over the last 10 years is in connectivity allowing modification of prescription over the wire. Baxter in July 2019 announced major investment in PD. Can we get online PD fluid production? #AspenKidney
Online peritoneal dialysate production overturns the current business model. He does not see that change. #AspenKidney
Wearable kidney? Sorbents present problems as well as the portable nature of a wearable device. Wahlstrom is skeptical. Fresenius invested 100 million dollars in sorbent technology that did not go anywhere. #AspenKidney
WAK is hemodialysis, requires blood access
AWAK is based on PD technology, still dependent on sorbents to regenerate dialysate
#AspenKidney
AWAK is based on PD technology, still dependent on sorbents to regenerate dialysate
#AspenKidney
He wants to make the case for PD. Better preservation of residual renal function. Better quality of life, cost-effective treatment. He thinks this is the best way to expand home therapy. #AspenKidney
It was difficult to grow PD despite major investments. Most effective was pre-ESRD education. But drop out was still a major problem. They improved starts but people stopped it. Fluid overload was a major reason for drop out. #AspenKidney
New technology to answer the problem of fluid overload in PD.
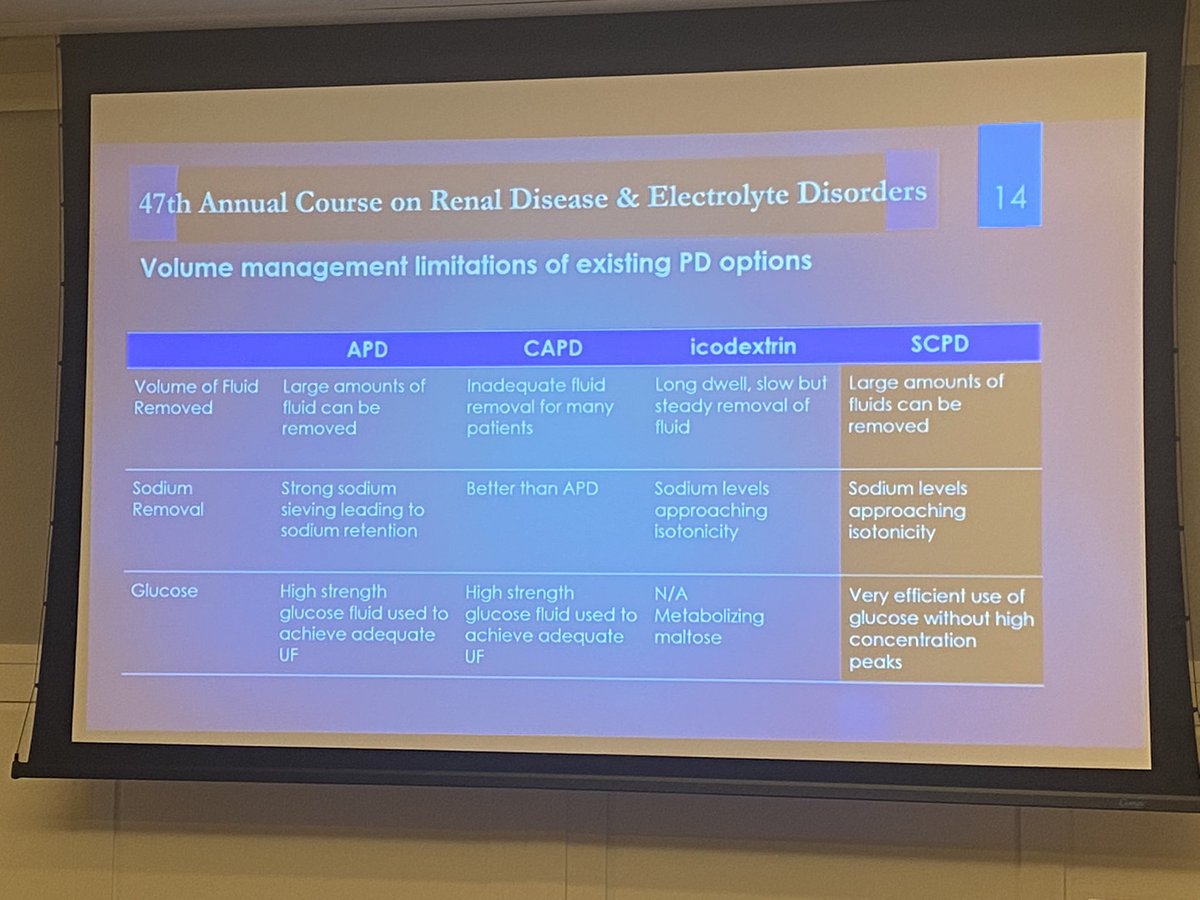
Steady Concentration Peritoneal Dialysis (SCPD)
Promises improved volume management
Limiting exposure of the peritoneum to high glucose concentrations
#AspenKidney
Steady Concentration Peritoneal Dialysis (SCPD)
Promises improved volume management
Limiting exposure of the peritoneum to high glucose concentrations
#AspenKidney
New device that supplement PD patients when they have fluid overload. They have a portable version for just fluid removal and small amount of solute removal. Working on a complete PD solution. #AspenKidney
The device works by continuously cycling the PD solution and adding glucose continuously to maintain osmotic gradient. #AspenKidney
May be an interesting device for CHF patients with fluid overload. #AspenKidney
The pitch #AspenKidney 
• • •
Missing some Tweet in this thread? You can try to
force a refresh