
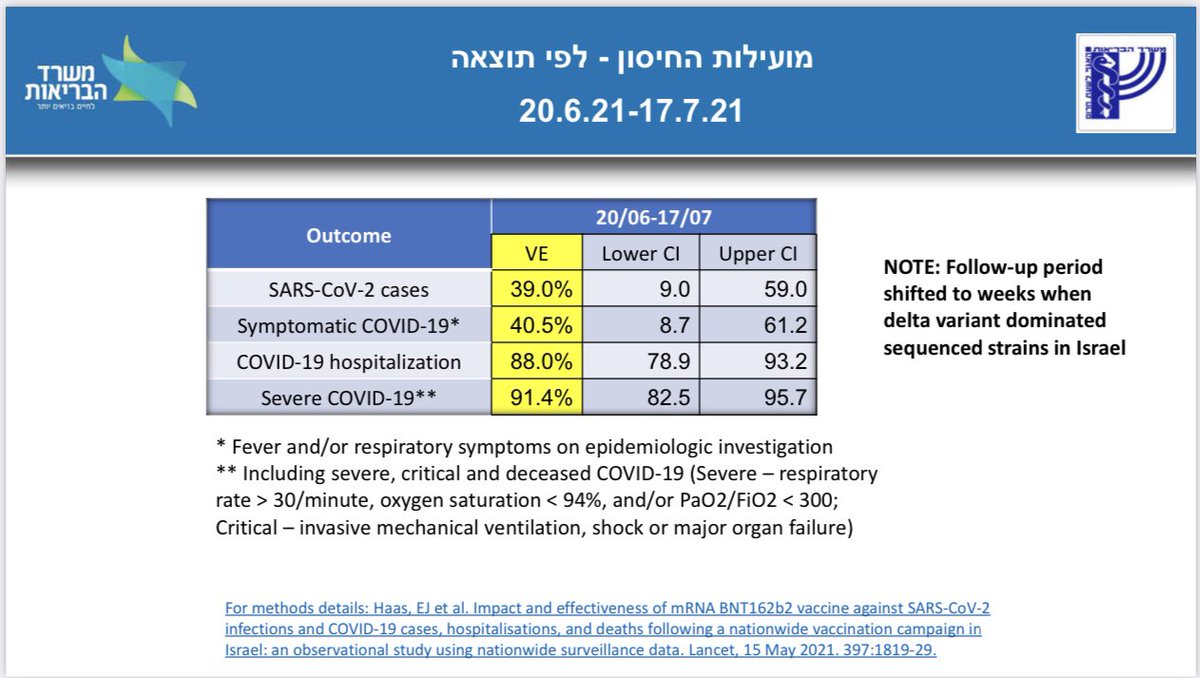
⚠️ANOTHER EFFICACY DROP—Not good—Israel 🇮🇱 Ministry of Health just released another vaccine efficacy update due to #DeltaVariant—only 39% Pfizer VE for #COVID19 infection, 40.5% for symptomatic, 88% for hospitalization, 91% for ICU/low oxygen/ death. More—waning efficacy too—🧵 

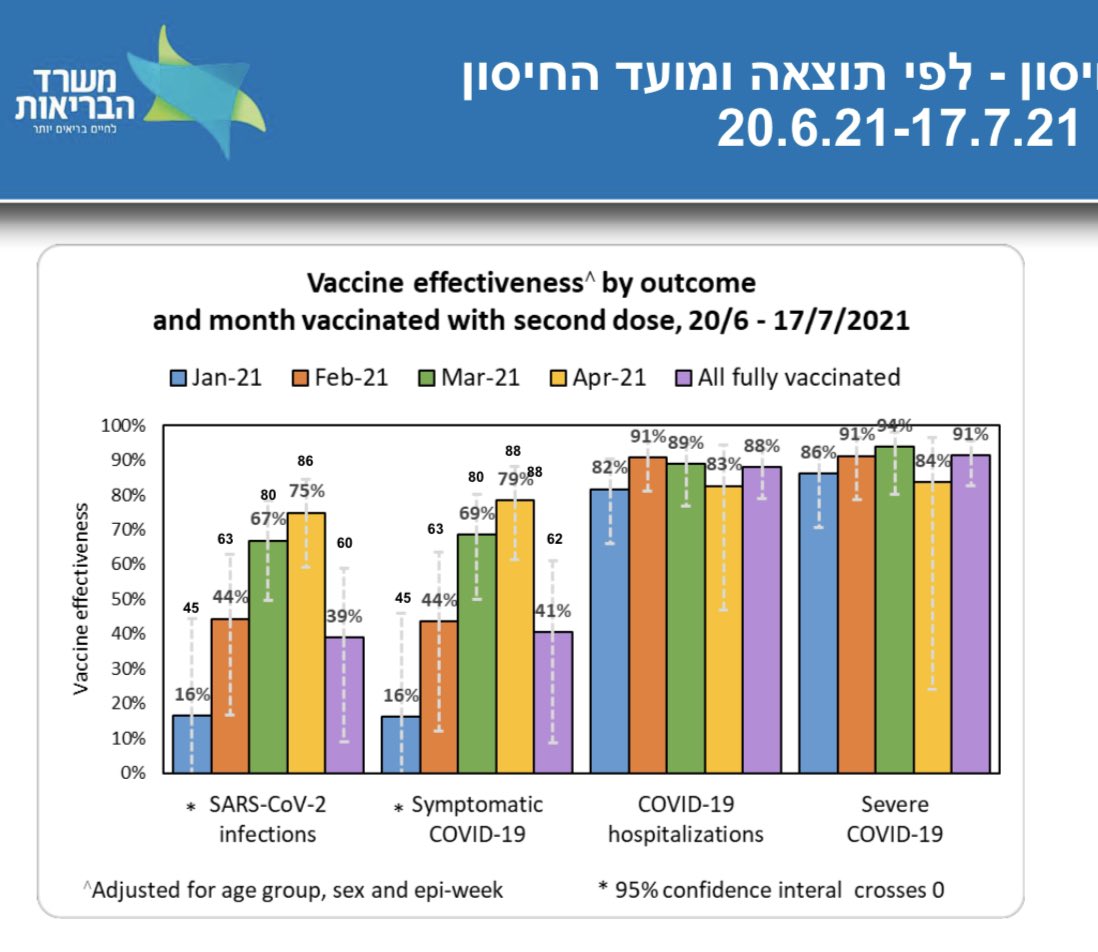
2) Gets worse, 🇮🇱 report also reveals waning potency, showing just 16% effectiveness against transmission among those 2nd-shot vaccinated in January, 44% VE if vaccinated in February, 67% VE if 2nd shot in March, 75% if vaccinated in April. Partly also age effect—but still bad.

3) I’m trying to find good things in the report—the 88% efficacy against hospitalization and 91% VE for severe #COVID19 death is good. But it is much weaker than the 93% reported 2 weeks ago for hospitalization, and 98% from May.
gov.il/BlobFolder/rep…
gov.il/BlobFolder/rep…
4) Let’s now look at breakthrough rates by when someone got their vaccination— you clearly clearly see than January vaccinated people currently have the most breakthrough per capita, followed by Feb… and so on. This is partly age (elderly vaxxed first) but possibly also waning.

5) This worrisome news is not just my perspective, the Israeli govt is quite worried too. They warn of “decreasing potency” i24news.tv/en/news/corona…
6) but is it just elderly effect in the weaker Jan/Feb potencies? Not sure… if you look at breakthrough rate in age 60+ versus 16-59, the 16-59 have similar if not higher breakthrough rate if comparing Jan vs Jan, Feb vs Feb of same month! That implies waning not just age.


7) here was 2 weeks ago… VE was 64% for preventing infection in early June. 94% in May. But now it’s 39-40%. Gee.
https://twitter.com/DrEricDing/status/1411973605609574401
8) Let me be clear—vaccines are amazing miracle. But we can’t just rely on just vaccines alone—must do other mitigation to get us out of the pandemic. Epidemiology models show that because #DeltaVariant so contagious, we *must must must* add masks and other NPI measures! ⬇️
https://twitter.com/GosiaGasperoPhD/status/1418699432036495363
9) Boosters—Biden WH Officials Now Expect Vulnerable Americans to Need Booster Shots—The growing consensus that at least some Americans will need a booster is tied in part to research suggesting that Pfizer’s vaccine is less effective after ~6 months. nytimes.com/2021/07/23/us/…
10) “Senior officials now say they expect that people who are 65 and older or who have compromised immune systems will most likely need a third shot from Pfizer or Moderna.”
11) “That is a sharp shift from just a few weeks ago, when the administration said it thought there was not enough evidence to back boosters yet.
12) “On Thursday, a key official at @CDCgov said the agency is exploring options to give patients with compromised immune systems third doses even before regulators broaden the emergency use authorization for coronavirus vaccines, a step that could come soon for Pfizer vaccine.
13) “Dr. Amanda Cohn, the chief medical officer of CDC immunizations division, told an advisory committee to the agency that officials were “actively looking into ways” to provide certain people access to booster shots “earlier than any potential change in regulatory decisions.”
14) there is some debate about the new 🇮🇱 ~40% efficacy data. Some say unvaccinated are tested more—true, but in that case, then we’d find relatively more cases in the unvaccinated, which would make the vaccine efficacy look BETTER, not worse (seen here).
timesofisrael.com/israeli-uk-dat…
timesofisrael.com/israeli-uk-dat…
15) Thus to rephrase—if unvaccinated are tested more than vaccinated, then we would fine more of the milder / asymptomatic infections in unvaccinated relatively, and that would make the vaccine efficacy look relatively higher, not lower. So that is unlikely to explain the VE dip.
16) another debate is that early vaccinations “reflect time that has passed since vaccination, but also… often people with health conditions and who are more prone to infection, such as the elderly.” We discussed this above—but again age isn’t explaining this—60+ & <60 similar.


17) Some others say “oh it’s a smaller dataset than UK”—yeah but it’s still VERY significant. Notice how the 95% confidence intervals’ lower bounds all exclude zero—and by comfortable cushion of certainly. And the 40% VE’s upper bound excludes 88% from 🏴 data. So these are diff.

18) also if we look at just the elderly age 60+ (stratification is one form of adjustment in epidemiology), we still see the jump up among the January vaccinated even among these elderly. This implies this is an effect by time (stratified adjusted roughly for age), not just age.

19) given the new data—in following the precautionary principle—we need to now urgently reconsider reimposing mask mandates again. @CDCDirector - it is time. Tick tock ⏰
https://twitter.com/DrEricDing/status/1408762971485003776
20) Whenever you see vaccine efficacy —keep in mind vaccines are amazing. But data suggest we need to also do both vaccines & public health measures (rather than rely on treatments). Iron lung machines was a good polio treatment, but it could never eradicate polio until vaccines.
https://twitter.com/DrEricDing/status/1418812448665214976
21) Welp—there’s discussions among epidemiologists now whether we can hold the #DeltaVariant down. With a R0=6 we can just barely. But with an R0=8 it’s much harder under 60% efficacy and 64% vaxxed. What is the estimated R0 range of Delta? 5-8 ➡️ more contagious than smallpox.
https://twitter.com/GosiaGasperoPhD/status/1418744819002732546
22) large numbers of experts (including @JeromeAdamsMD) now support masks even if vaccinated. @CDCDirector needs to update mask rules ASAP now in light of the new data^
https://twitter.com/apoorva_nyc/status/1418251783315542021
23) #DeltaVariant cases ➡️ hospitalizations. Period. The “link is broken” disinformation machine is running wild that they aren’t correlated anymore. Completely false. Do not fall for that nonsense. Hospitalizations rising in UK and US and Israel.
https://twitter.com/ProfColinDavis/status/1418602366799163392
24) Vaccines are a miracle but we need other mitigation against #DeltaVariant. Iceland is one of the most heavily vaccinated countries in the world… but yet… and yes their ICUs are filling up too.
https://twitter.com/equibotanica/status/1418820007975342081
25) sure looks like we are headed to 3rd shot boosters… both the original vaccine booster as well as a #DeltaVariant tailored booster according to Pfizer. Their internal data also shows waning. finance.yahoo.com/news/pfizer-bi…
26) This is not good. Even under rosy optimistic scenarios, containing #DeltaVariant was already hard. But it’s not easy…. see details 🧵
https://twitter.com/DrEricDing/status/1419079452718415875
27) REMINDER— even *mild* COVID still leads to drop in intelligence according to UK 🇬🇧 studies on #COVID19 survivors. The cognitive drop is stronger as it gets more severe, but even significant in the mild cases too! Avoid infection not just hospitalization!
https://twitter.com/DrEricDing/status/1419873294023602176
28) Another reminder: mild breakthrough #COVID19 infections can still cause transmission. This is why we mask even if vaccinated! It slows and helps stop the spread. Mask and vaccinate … not just ‘or’.
https://twitter.com/DrEricDing/status/1420114915549974528
29) we are mostly pretty certain boosters are coming… the issue is not if but when… and who first.
https://twitter.com/DrEricDing/status/1420240803079892995
30) Pfizer reports 12% symptomatic efficacy after 4 months. But it was mostly data from the pre-#DeltaVariant era. Just FYI.
https://twitter.com/DrChoueiri/status/1420491128634236929
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















