We can’t vaccinate our way out of the pandemic.
We need both: Vaccines AND Public Health (PH) measures.
It was barely possible w/ original variant (A). W/ Delta, both PH measures and vaccines became less effective (B). But combined – they may still work.
Theoretical model:
1/
We need both: Vaccines AND Public Health (PH) measures.
It was barely possible w/ original variant (A). W/ Delta, both PH measures and vaccines became less effective (B). But combined – they may still work.
Theoretical model:
1/


Even if vaccines are only 60% efficient against transmission & only 75% eligible people (64% total) get vaccinated, by combining PH measures & vaxx we may still be able to control the spread (C). Barely.
But…
2/
But…
2/

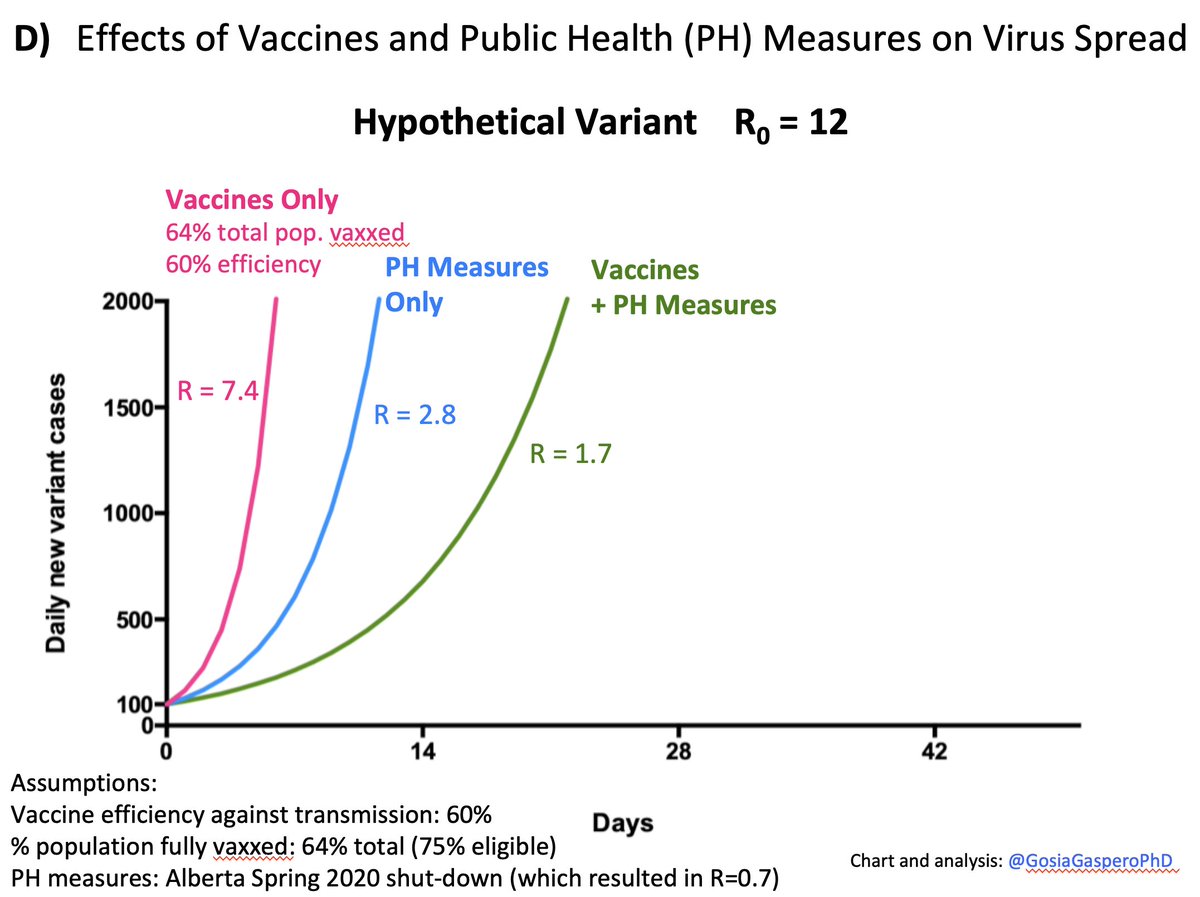
But if by allowing the reckless spread we culture a variant 2x more transmissible than Delta → our current strategy (i.e. acting only when ICUs get full) won’t work anymore.
Our tools: PH measures & vaccines will not be effective enough to quickly halt the exp. growth (D)
3/
Our tools: PH measures & vaccines will not be effective enough to quickly halt the exp. growth (D)
3/

Delta is our wake up call.
Our tools still (although barely) work against it.
We urgently need local and global COVID elimination strategy.
@WHO @DrMikeRyan @mvankerkhove @GovCanHealth @CPHO_Canada
fin/
Our tools still (although barely) work against it.
We urgently need local and global COVID elimination strategy.
@WHO @DrMikeRyan @mvankerkhove @GovCanHealth @CPHO_Canada
fin/
Appendix:
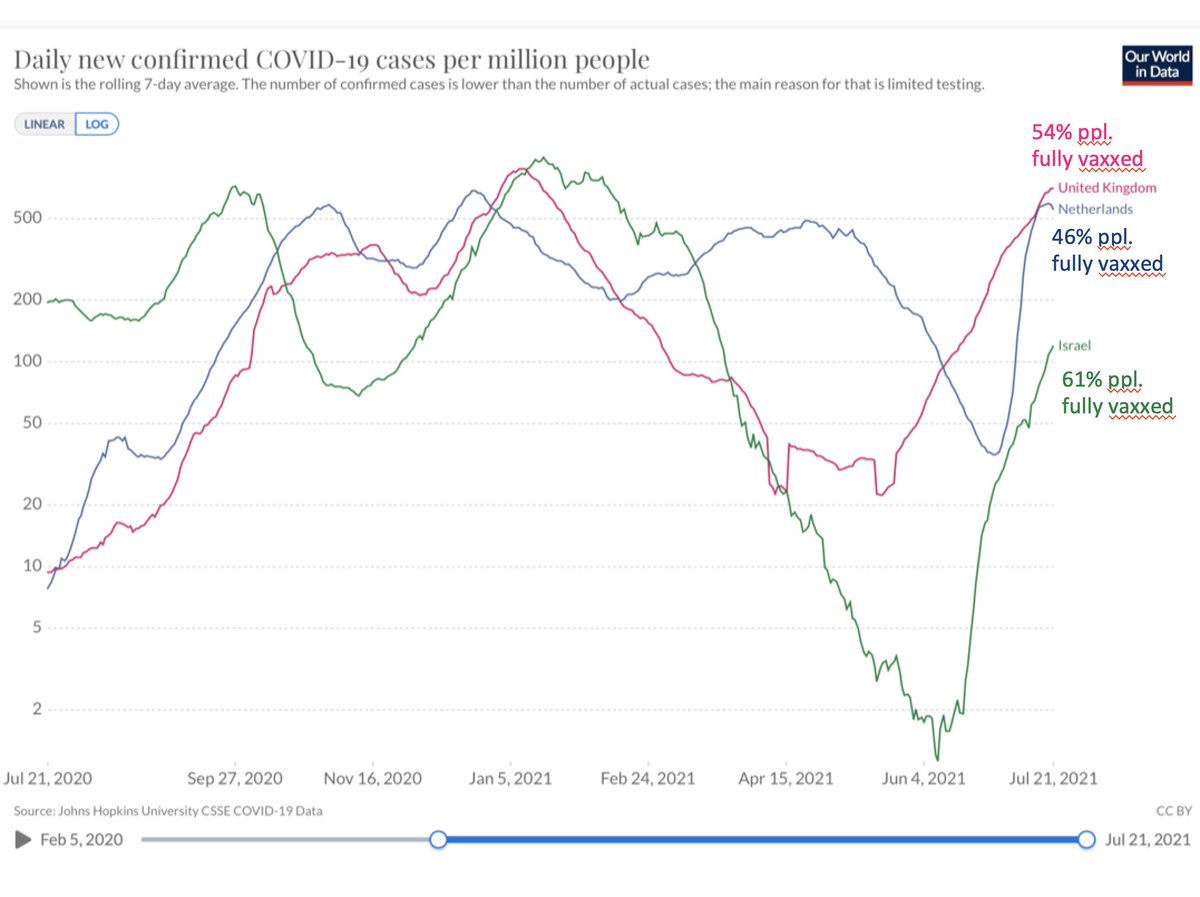
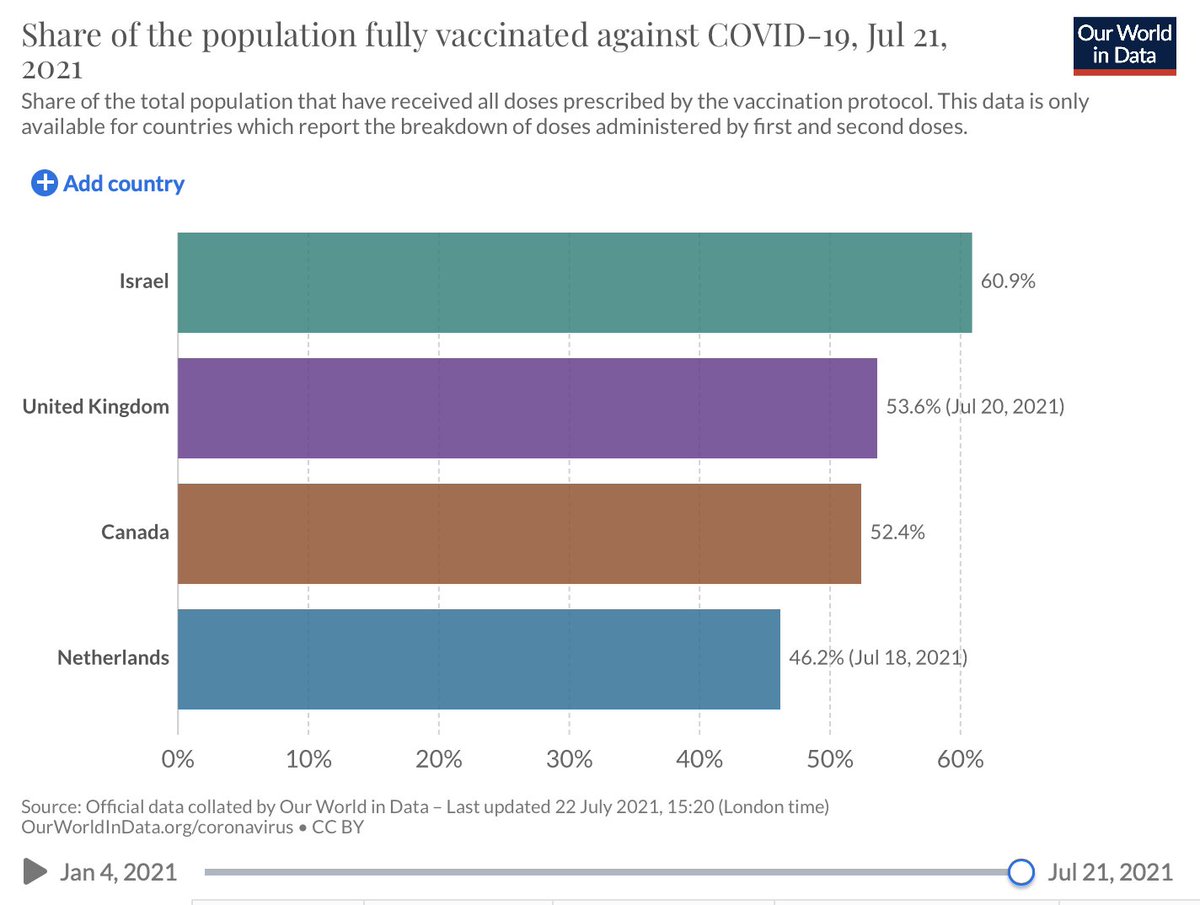
Real life experiment demonstrating that vaccinations *alone* don't stop Delta growth. UK (54% total population fully vaxxed), Israel (61% pop fully vaxxed, w/ Pfizer), Netherlands (46% pop fully vaxxed) 👇
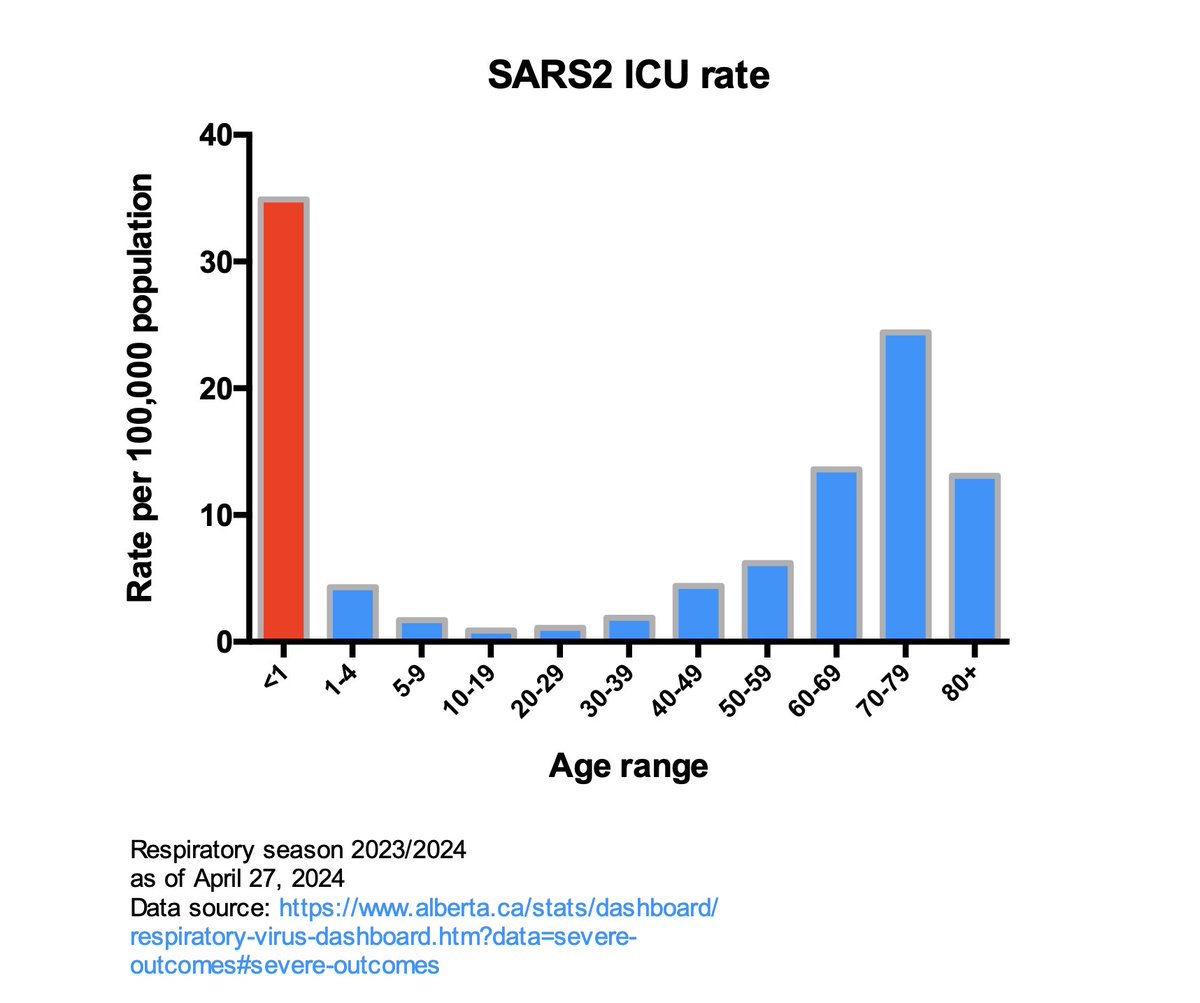
Plus: When there are cases → there are hospitalizations.
Real life experiment demonstrating that vaccinations *alone* don't stop Delta growth. UK (54% total population fully vaxxed), Israel (61% pop fully vaxxed, w/ Pfizer), Netherlands (46% pop fully vaxxed) 👇
Plus: When there are cases → there are hospitalizations.

Addition to tweet #3. We don't need to wait for a variant w/ R0 = 12.
A variant w/ R0 = 8 might be already uncontrollable.
H/t @DGBassani
A variant w/ R0 = 8 might be already uncontrollable.
H/t @DGBassani

• • •
Missing some Tweet in this thread? You can try to
force a refresh