
Delighted to share this in @TheLancet, with @EdjCarr. Neutralisation of live SARS-CoV-2 (+variants) in haemodialysis patients after BNT162b2 or ChAdOx-1.
thelancet.com/journals/lance…
Funding @Kidney_Research @NKF_UK @PKDCharity @KidneyWales
Thanks to patients taking part. 1/n
thelancet.com/journals/lance…
Funding @Kidney_Research @NKF_UK @PKDCharity @KidneyWales
Thanks to patients taking part. 1/n
2/n Context-1: Haemodialysis [HD] patients respond poorly to traditional vaccines.
Hepatitis B vaccine is reformulated
Pneumococcal boosters are recommended
Influenza vaccine responses are attenuated
Context-2: HD patients either excluded from Phase III trials, or not reported.
Hepatitis B vaccine is reformulated
Pneumococcal boosters are recommended
Influenza vaccine responses are attenuated
Context-2: HD patients either excluded from Phase III trials, or not reported.
3/n Context-3: HD patients clinically vulnerable: CFR ~25% in first wave.
Context-4: HD patients could not shield. They had to come to hospital 3x / week for HD.
Context-4: HD patients could not shield. They had to come to hospital 3x / week for HD.
4/n Massive UK effort to vaccinate HD at speed … e.g. this on weekends
@kidneydoc101 @mkwillicombe and many around UK.
And for our cohort:
https://twitter.com/kidneydoc101/status/1348786584502546435?s=20
@kidneydoc101 @mkwillicombe and many around UK.
And for our cohort:

5/n Lots of nephrologists have realised Ab worth checking out in HD... reviewed kireports.org/article/S2468-…
and nephjc.com/news/covid-vac…
and nephjc.com/news/covid-vac…
https://twitter.com/hswapnil/status/1425761295006109696

6/n Almost all of the above studies measure spike-binding Ab by ELISA (or similar). Neutralising Ab are best correlate of protection, as shown by others. nature.com/articles/s4159…
7/n @TheCrick we have established a high-throughput live virus microneutralisation assay. Important results published already:
doi.org/10.1016/S0140-…
doi.org/10.1016/S0140-…
doi.org/10.1016/S0140-…
doi.org/10.1016/S0140-…
https://twitter.com/DavidLVBauer/status/1400582718166122499?s=20
8/n Looking at the results: Sera from 178 patients, before dose 1 and median 33 days after dose 2.
For patients with prior COVID infection, both BNT162b2 and AZD1222 induced high nAb titres. Both vaccines generate generous median nAb titres.
For patients with prior COVID infection, both BNT162b2 and AZD1222 induced high nAb titres. Both vaccines generate generous median nAb titres.
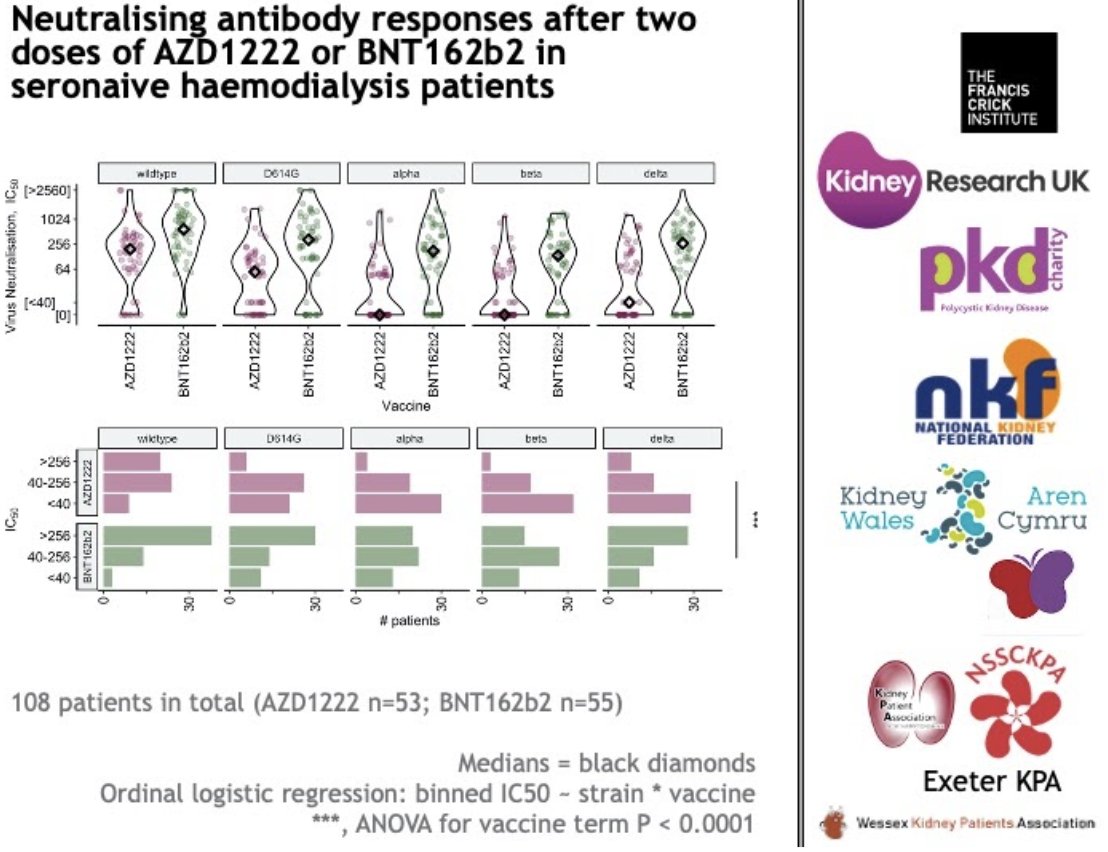
9/n However, we had 108 patients with no evidence of prior exposure [either by Ab testing or by PCRs] and found substantially differing responses between the two vaccines, particularly against VOCs. Median for AZ vs Delta is below quantitative range.
10/n When we compared this to responses in healthy individuals we found that the mRNA vaccine gives comparable nAbs to healthy individuals - an unexpected success given attenuated HD responses to classic vaccines.

11/n Implications of our study:
– mRNA vaccines (e.g. for flu) may be really useful in HD
– AZD recipients without prior infection, may be vulnerable to infection
– Three rounds of spike encounter gives good nAb titres in HD.
– mRNA vaccines (e.g. for flu) may be really useful in HD
– AZD recipients without prior infection, may be vulnerable to infection
– Three rounds of spike encounter gives good nAb titres in HD.
12/n Third doses for CEV patients in the UK have been announced in principle gov.uk/government/pub…
Not yet finalised + no details yet on vaccine formulation or timing. Our data help those decisions.
Not yet finalised + no details yet on vaccine formulation or timing. Our data help those decisions.
13/n A third dose for some CEV groups looks to be needed *to complete a successful first course of vaccination*.
We believe a third dose for some CEV groups is equitable. This is not really similar to a ‘booster’ to an already adequate primary response (e.g. young HCWs).
We believe a third dose for some CEV groups is equitable. This is not really similar to a ‘booster’ to an already adequate primary response (e.g. young HCWs).
14/n Globally the best vaccine for HD patients is still the vaccine you can get earliest. Our study should not dissuade people from vaccination with adenoviral vectored vaccines where that's best local choice.
15/n Amazing team: @MaryYiWeiWu @dremmacbw @DavidLVBauer @CharlesSwanton @LabGandhi @salama_alan @mkwillicombe @DrMattGB @stephenmcadoo @gavinpaulkelly @rezamotallebov @drpaddymark @Sush_Shankar @drmattgb @RBillany @drpaddymark ++ more off Twitter (apologies if we missed you!)
16/16 This is the 'trailer' (178 patients), with 'feature length' to come (≈1k patients). Lots more to come. Many thanks once again to patients and their families.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



