While there is so much established about CAC..
for @Heart_SCCT Prevention Symposium, I was asked by @RonBlankstein to talk about
"what's next for CAC Testing in 2021 (and beyond)?"
What are the main applications in the future?
@miguelcainzos23 @jaideeppatelmd
for @Heart_SCCT Prevention Symposium, I was asked by @RonBlankstein to talk about
"what's next for CAC Testing in 2021 (and beyond)?"
What are the main applications in the future?
@miguelcainzos23 @jaideeppatelmd

#1 CAC has come a long way
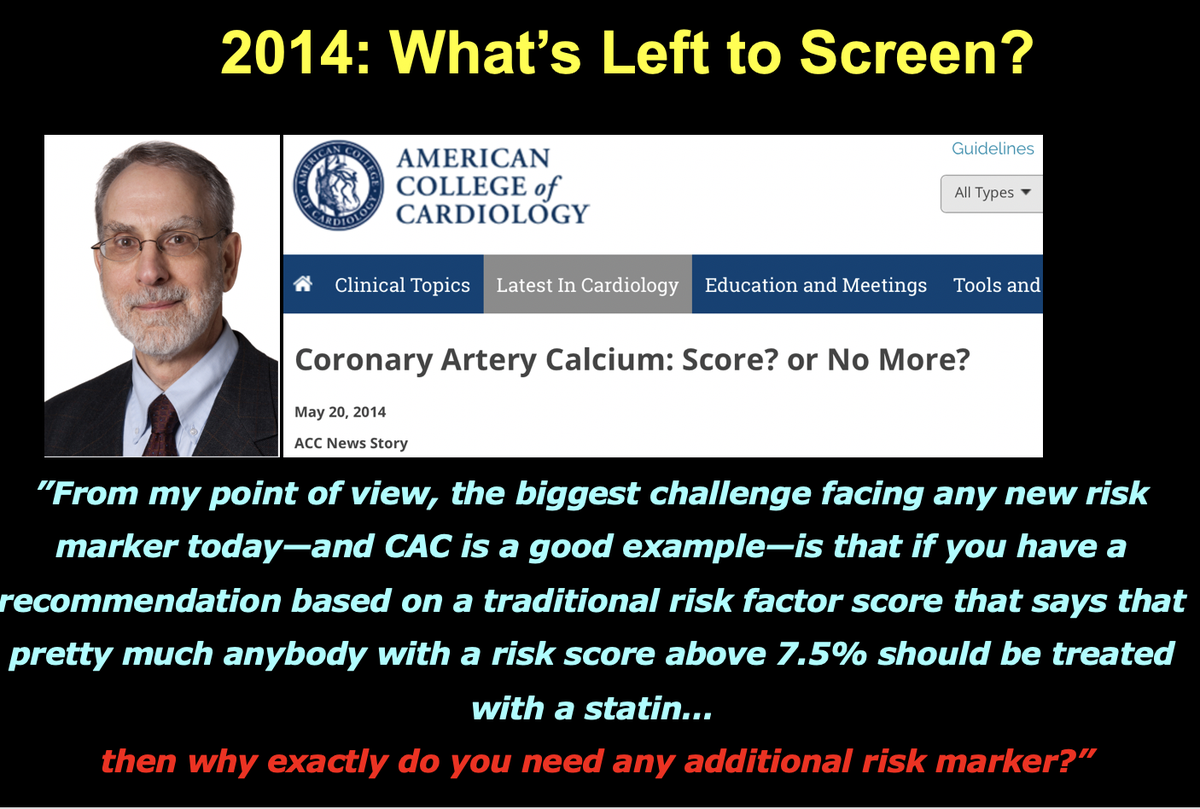
-evolving to the needs of the past decade from screening test to a SDM tool
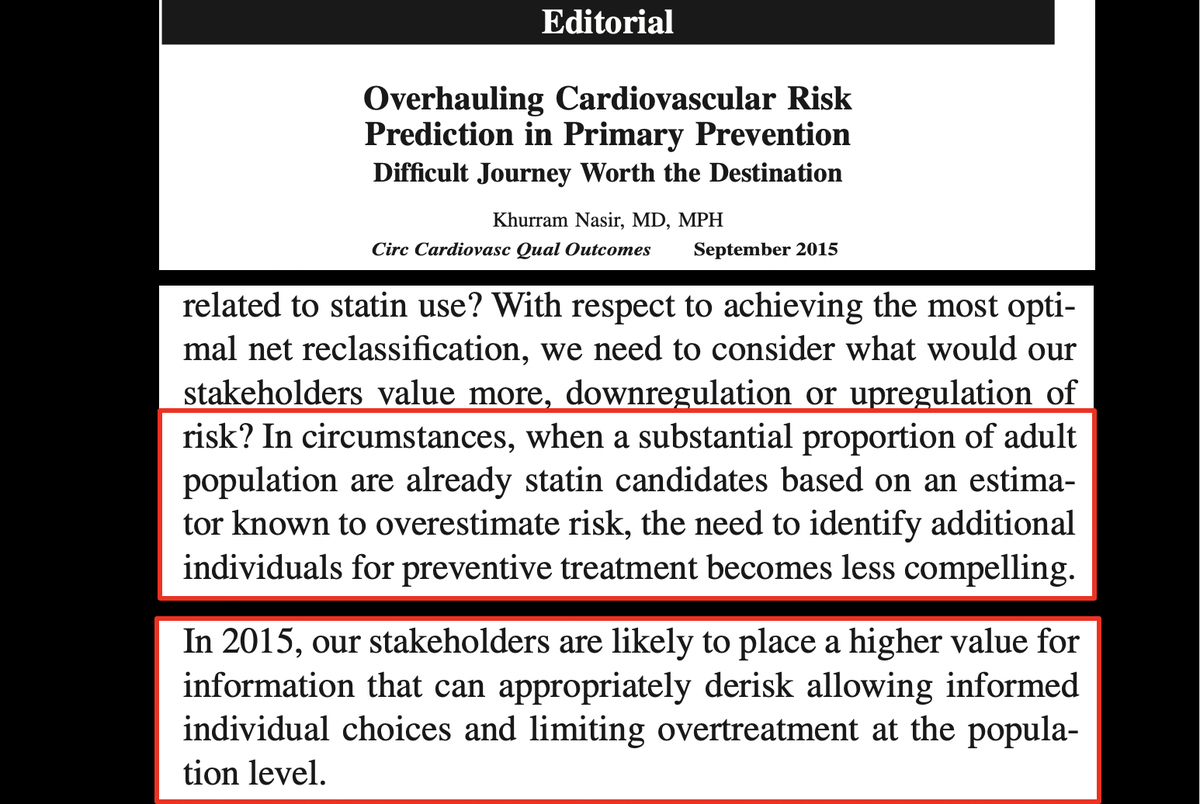
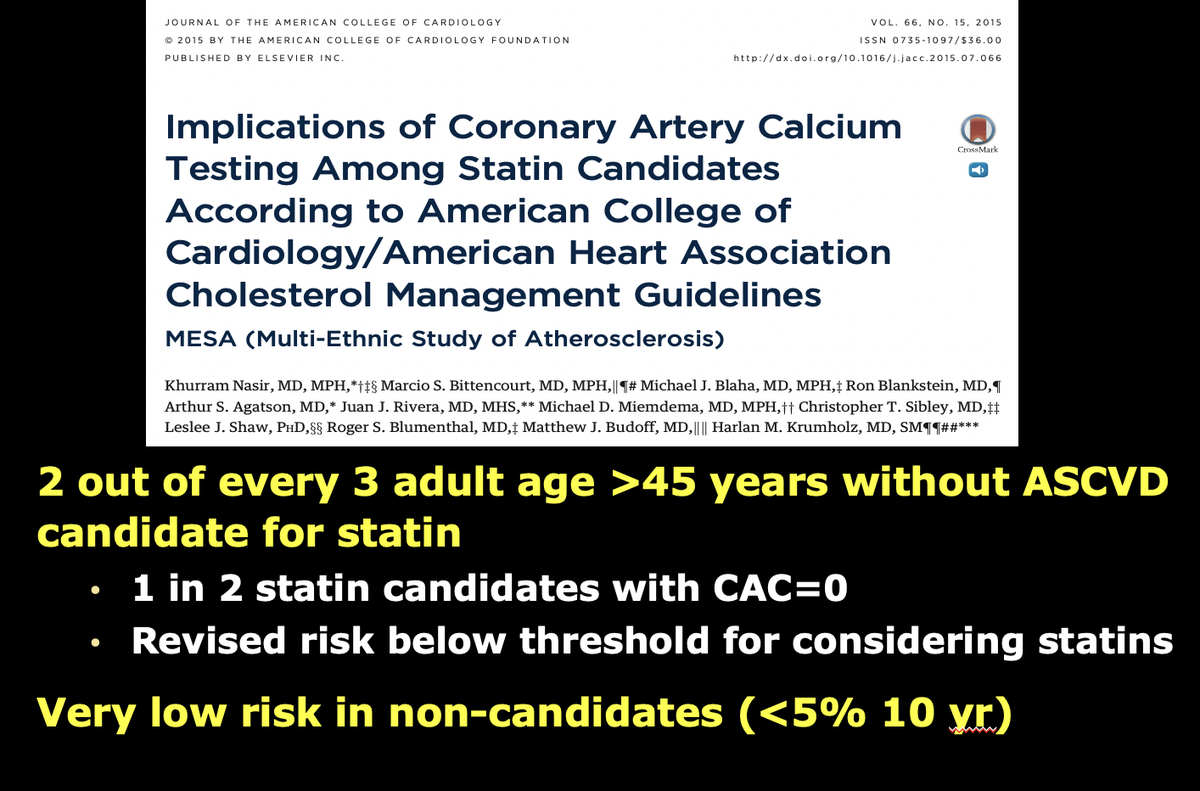
-best tie breaker, adding the dimension of de-risking
-cost-effective and reassuring ok to avoid treatment
-cautiously approved by ACC/AHA guidelines
@Heart_SCCT
-evolving to the needs of the past decade from screening test to a SDM tool
-best tie breaker, adding the dimension of de-risking
-cost-effective and reassuring ok to avoid treatment
-cautiously approved by ACC/AHA guidelines
@Heart_SCCT




#2
Looking forward, beyond established role as decision tool for statins and possibly ASA
we need to think beyond what the future may hold for CAC testing.
While I have a list of at least 10 applications, I will share today the top 5 immediate future roles for CAC testing
Looking forward, beyond established role as decision tool for statins and possibly ASA
we need to think beyond what the future may hold for CAC testing.
While I have a list of at least 10 applications, I will share today the top 5 immediate future roles for CAC testing

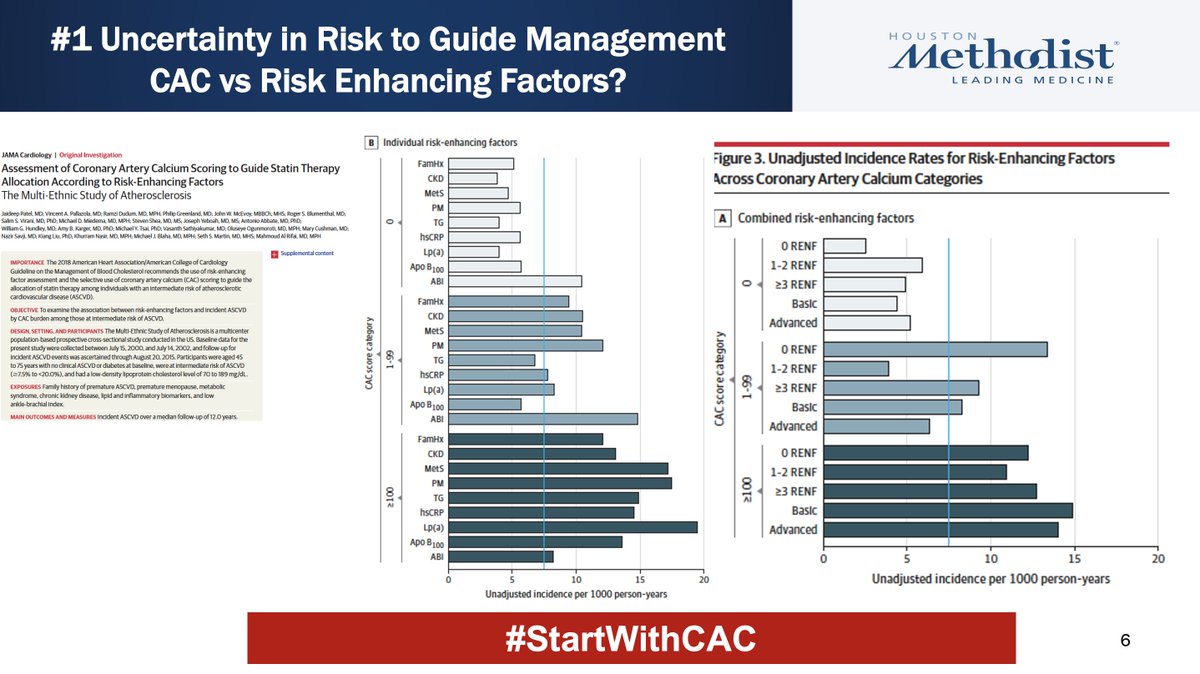
#3 First, If uncertain of risk, guidelines suggest start with risk enhancing factor vs CAC
Evidence for this rec? None
Now @jaideeppatelmd show even with multiple REF, CAC zero in 40%->reclassified risk low below statin threshold
CAC superior to REF
Next time #StartWithCACFirst
Evidence for this rec? None
Now @jaideeppatelmd show even with multiple REF, CAC zero in 40%->reclassified risk low below statin threshold
CAC superior to REF
Next time #StartWithCACFirst
#4
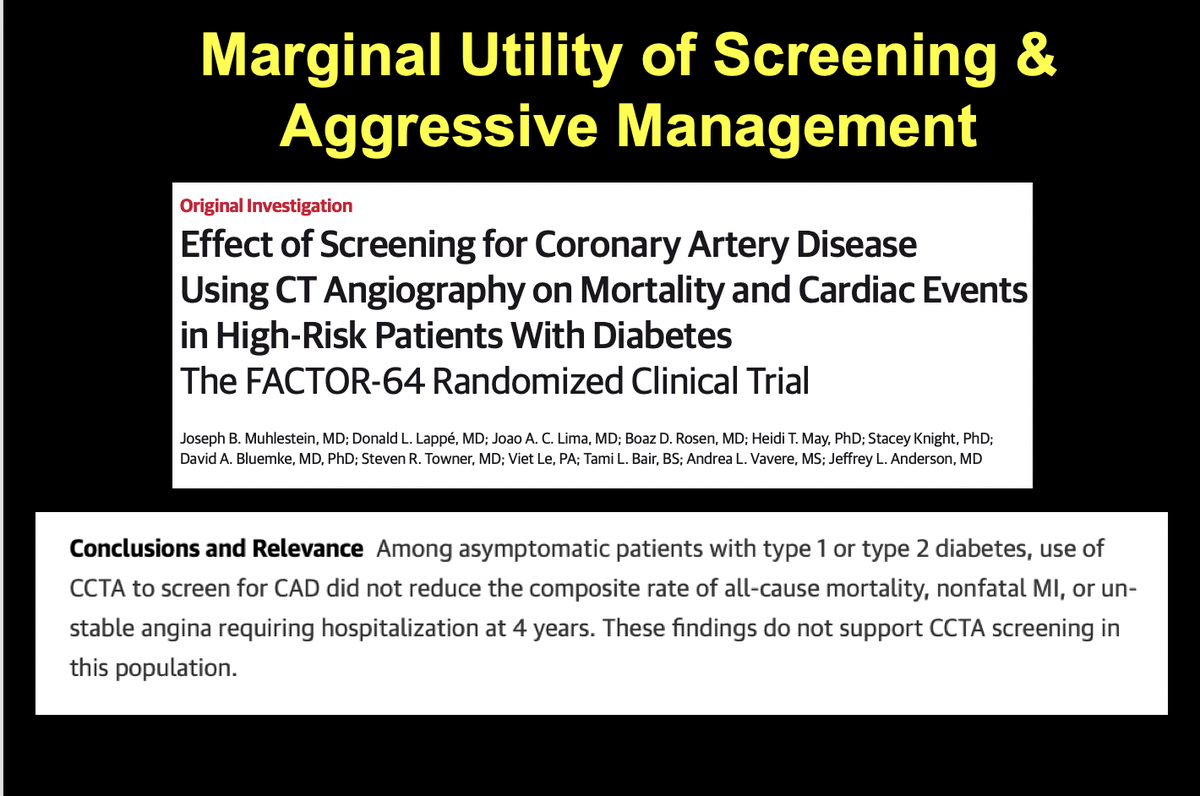
Second, CAC not recommended for risk stratification among DM
Why? Not clear
But now evidence suggest not all DM equal
-#PowerOfZero means flexible treatment
-#HighCACCVDEquivalent secondary prevention measures should be applied to them.
Second, CAC not recommended for risk stratification among DM
Why? Not clear
But now evidence suggest not all DM equal
-#PowerOfZero means flexible treatment
-#HighCACCVDEquivalent secondary prevention measures should be applied to them.


#5 Similarly with LDL>190 or FH, guidelines don't recommend CAC
Both groups are not homogenous
#PowerOfZero reassuring (possible no PCSK9i)
CAC>100 very high risk->most aggressive management
CAC passes another test->societal resource allocation and informed choices
Both groups are not homogenous
#PowerOfZero reassuring (possible no PCSK9i)
CAC>100 very high risk->most aggressive management
CAC passes another test->societal resource allocation and informed choices


# 6 Third, With growing options addressing residual risk beyond statins reserved for CVD pt @miguelcainzos23 and I believe CAC testing most efficient and cost tool for future value based RCT design scaling in primary prevention
targeted approach->better likelihood of adoption
targeted approach->better likelihood of adoption

#7, Fourth To-date focus of CAC testing has been among non young
Now with 3 major studies showing a focused approach targeted almost 25-35% young have CAC & increased risk
In this regard, we feel, Age is just a number and it’s time to lower the bar for CAC testing
Now with 3 major studies showing a focused approach targeted almost 25-35% young have CAC & increased risk
In this regard, we feel, Age is just a number and it’s time to lower the bar for CAC testing

#8, Fifth With undeniable evidence, I sincerely hope upcoming chest pain guidelines will upgrade the role of #PowerOfZero as gatekeeper by listening to Wayne Gretzky—probably greatest hockey player of all time—“I skate to where the puck is going to be, notwhere it has been.”

Future?
#StartWithCACFirst if uncertain of risk for statins
#NotAllHighRiskSame Strong CAC role in DM, LDL>190 & #HEFH
#DoubleEnrichment targeted values based clinical trials
#AgeIsJustaNumber Screen high risk young individuals
#CACgatekeeperLowRiskChestPain Cant want more
#StartWithCACFirst if uncertain of risk for statins
#NotAllHighRiskSame Strong CAC role in DM, LDL>190 & #HEFH
#DoubleEnrichment targeted values based clinical trials
#AgeIsJustaNumber Screen high risk young individuals
#CACgatekeeperLowRiskChestPain Cant want more

@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh