just finished nights on call, and found that a toxic triad of RSV, rhinovirus and SARS-CoV-2 is starting to stretch the Scottish hospital I work in to its limits
it's only August
what went wrong? 🧵1/n
it's only August
what went wrong? 🧵1/n
Problem 1. We failed to contain SARS-CoV-2. 2/n 

This is a Problem for 3 reasons.
Firstly, there are the (very) small number of children with serious SARS-CoV-2 infection. 3/n
Firstly, there are the (very) small number of children with serious SARS-CoV-2 infection. 3/n
Secondly, as community prevalence rises, so does the number of children being admitted with incidental SARS-CoV-2 infection. These children still require cubicles and full infection control measures, and this adds to the nursing burden for their care. 4/n
Thirdly, and most importantly, as prevalence rises, more and more nurses and doctors are forced to self-isolate putting pressure on already tight rotas. 5/n
Problem 2. Rhinovirus arrives with the start of the school term (mid-August in Scotland).
Rhinovirus spreads rapidly in schools, which are in the process of relaxing social distancing measures. 6/n
Rhinovirus spreads rapidly in schools, which are in the process of relaxing social distancing measures. 6/n
Hospitals see a spike in rhinovirus related pre-school wheeze every year at the start of term (August in Scotland, September in England).
We saw this spike in 2020 at the start of the last school year, even with social distancing measures implemented. 7/n
We saw this spike in 2020 at the start of the last school year, even with social distancing measures implemented. 7/n
The start of this school term has been business as usual @dgurdasani1. 8/n
In addition to wheeze in preschool and school children, rhinovirus can cause severe bronchiolitis in infants, and serious lower respiratory tract infections in children with co-morbidities, who often need HDU or PICU care as a result. Not "just a cold". 9/n
Normally then there is then a bit of a lag until RSV infections starts to rise in September/October. However this year England has been incubating RSV over the summer for Scotland, and rates here were rising as schools re-started. 10/n
Which leads to Problem 3. As well as arriving at the worst possible time, RSV is affecting not only infants but older children. 11/n
RSV is highly infectious, and pre-pandemic most children had been infected by the age of two. This means that every year a high proportion of children acquired a degree of immunity for the subsequent season. 12/n
However there has been no RSV for the last 18 months (eurosurveillance.org/content/10.280…), so there is a younger cohort with no immunity, and another older cohort with reduced immunity. 13/n
This results in the usual numbers of small babies with severe disease.
But also older children presenting with RSV lower respiratory tract infections that we have no accepted approach for triaging and treating. 14/n
But also older children presenting with RSV lower respiratory tract infections that we have no accepted approach for triaging and treating. 14/n
Although thanks to the BIDS study (pubmed.ncbi.nlm.nih.gov/26382998/) we are comfortable in discharging infants who can maintain saturations over 90% in air ... 15/n
... there is no consensus on a safe limit for older children, which means that we end up admitting these children for days whilst we wait for their saturations whilst asleep to rise above 92% @mairi_stark 16/n
There is a lot of debate about the risk to children from COVID-19 & whether they should be vaccinated.
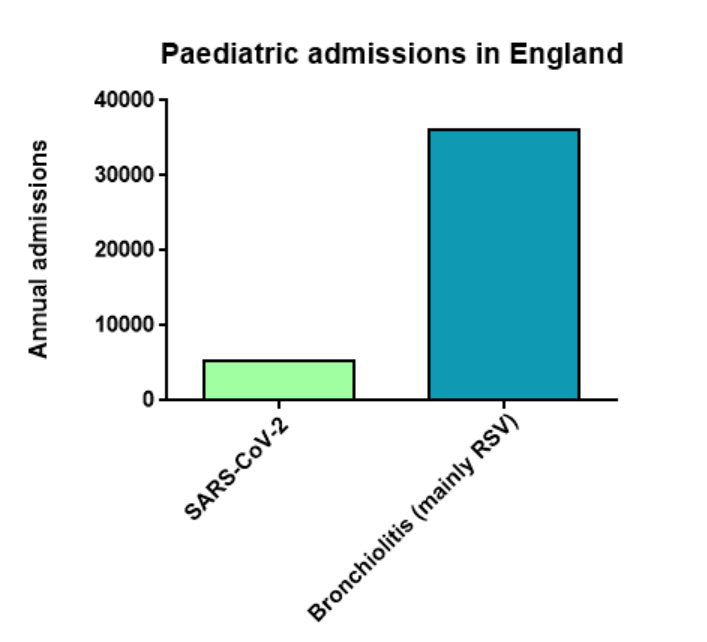
The risk to children from rhinovirus/RSV is well understood & much higher than that from SARS-CoV-2.
The risk to children from an overwhelmed health system is also real. 17/n
The risk to children from rhinovirus/RSV is well understood & much higher than that from SARS-CoV-2.
The risk to children from an overwhelmed health system is also real. 17/n
My colleagues in the Emergency Department look burnt out and exhausted. 18/n
My nursing colleagues fret about the weeks & months to come. 19/n
We need Solutions, not Problems, right? 20/n
So what can we do? 21/n
We can carry out research to understand these new patterns of disease.
Soon the BronchStart study (wellcomeopenresearch.org/articles/6-120) will release a live dashboard of bronchiolitis/LRTI cases across the United Kingdom and Ireland in real time @MyMicroreact . 22/n
Soon the BronchStart study (wellcomeopenresearch.org/articles/6-120) will release a live dashboard of bronchiolitis/LRTI cases across the United Kingdom and Ireland in real time @MyMicroreact . 22/n

It will collect data on age of presentation, clinical features, and management, and help us make sense of this 2021 disease. 23/n
England should look at Scotland and think about the consequences of returning to business as usual for schools in the coming weeks @GavinWilliamson . 24/n
We need guidance on how we can safely assess and treat older children with RSV- do they really need prolonged hospital admission? 25/n
We have a SARS-CoV-2 vaccine for 12-15 year olds. We already vaccinate younger children for influenza mainly to protect the elderly and vulnerable.
Perhaps we should reframe vaccinating younger teenagers as a way to protect their education & the community more generally. 26/n
Perhaps we should reframe vaccinating younger teenagers as a way to protect their education & the community more generally. 26/n
We learnt how to shield our most vulnerable adults during the pandemic.
We should pivot towards doing the same for the most vulnerable children- the youngest infants & those born preterm. 27/n
We should pivot towards doing the same for the most vulnerable children- the youngest infants & those born preterm. 27/n
Limiting social interactions for the first few months of life and rigorous attention to hygiene could make a big difference. 28/n
In a couple of years we could be through the worst of this. 29/n
1. We'll have a COVID-19 vaccine for children of all ages.
2. We'll have an effective maternal and infant vaccine for RSV.
3. mRNA technologies offer the promise of a vaccine for the most virulent strains of rhinovirus. 30/n
2. We'll have an effective maternal and infant vaccine for RSV.
3. mRNA technologies offer the promise of a vaccine for the most virulent strains of rhinovirus. 30/n
But the big question is- will we get there without needing a circuit breaker(s) for these childhood viruses?
#notjustavirus
END
#notjustavirus
END
• • •
Missing some Tweet in this thread? You can try to
force a refresh