
as lockdown is lifted across the UK and Ireland, what could happen in paediatric emergency departments and hospitals this summer? a 🧵1/n
firstly, some context
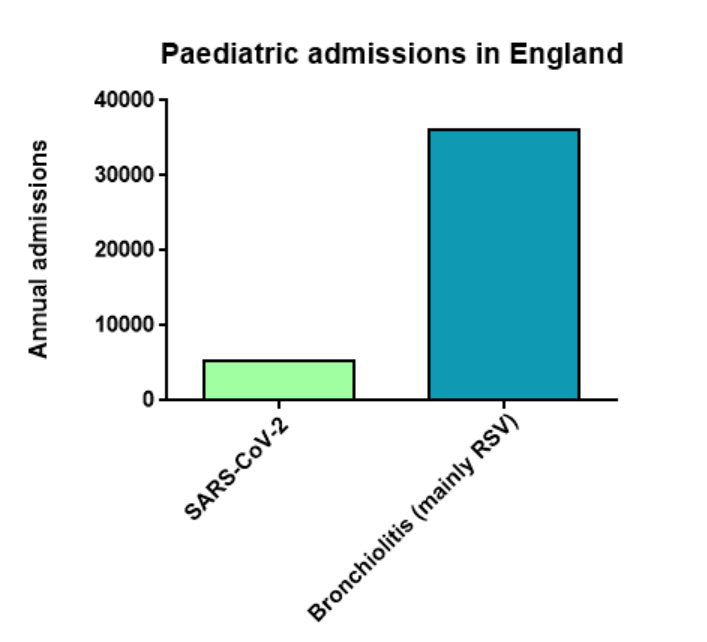
in the first year of the pandemic, there were 5,336 hospital admissions associated with a positive SARS-CoV-2 test in children in England
in the first year of the pandemic, there were 5,336 hospital admissions associated with a positive SARS-CoV-2 test in children in England
https://twitter.com/LongCovidKids/status/13744324988185763882/n

but ...
in a typical year in England, there are ~36,000 admissions for bronchiolitis (mainly caused by Respiratory Syncytial Virus, RSV) in infants under the age of 1 thorax.bmj.com/content/75/3/2… 3/n
in a typical year in England, there are ~36,000 admissions for bronchiolitis (mainly caused by Respiratory Syncytial Virus, RSV) in infants under the age of 1 thorax.bmj.com/content/75/3/2… 3/n
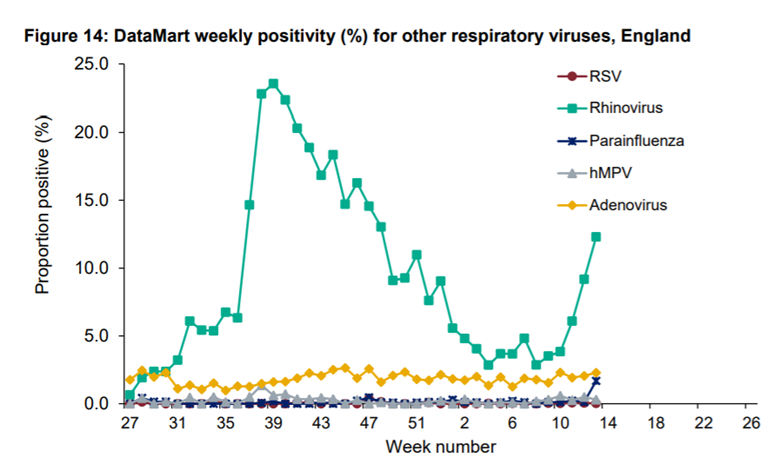
the pandemic saw an almost total disappearance of RSV across the UK gov.uk/government/sta… @PHE_uk 4/n
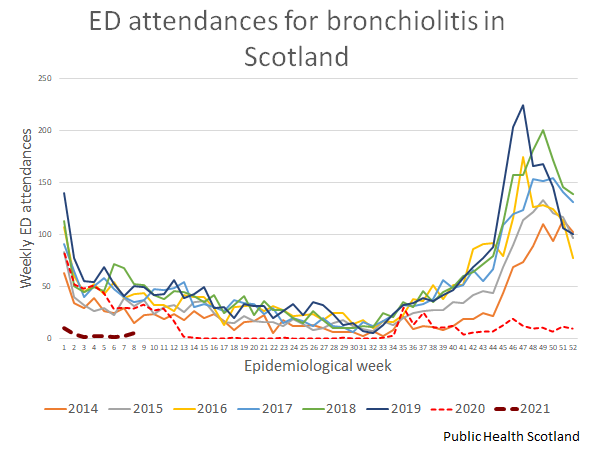
this was reflected in emergency department attendances for bronchiolitis across Scotland
in contrast to a usual winter peak, there were very few attendances, most likely representing ongoing rhinovirus circulation (@P_H_S_Official data) 5/n
in contrast to a usual winter peak, there were very few attendances, most likely representing ongoing rhinovirus circulation (@P_H_S_Official data) 5/n
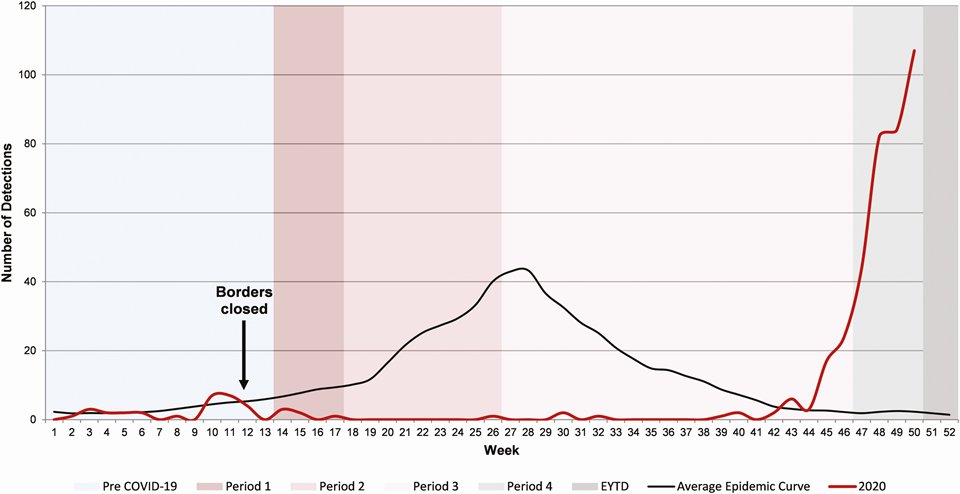
much of the Southern Hemisphere saw a similar pattern
but what happened when lockdown was released?
in Western Australia the peak was larger than the normal winter peak academic.oup.com/cid/advance-ar… 6/n
but what happened when lockdown was released?
in Western Australia the peak was larger than the normal winter peak academic.oup.com/cid/advance-ar… 6/n
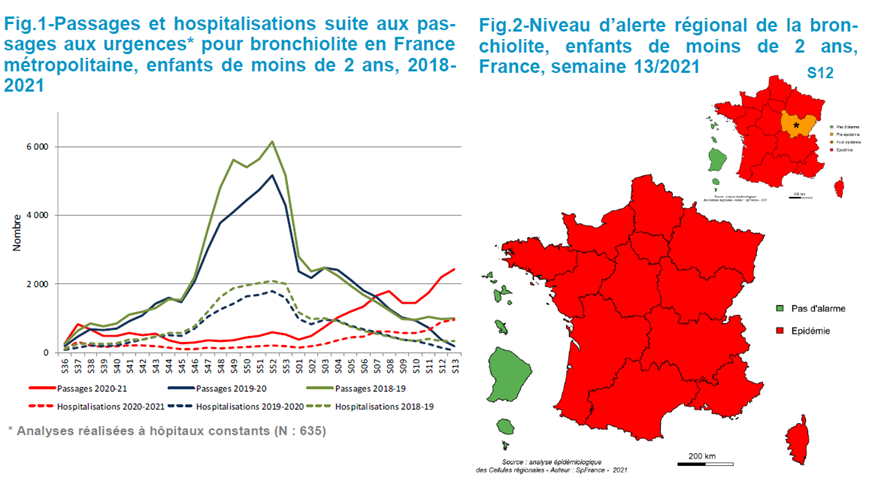
in France, where schools have remained open throughout the winter and into spring, there is an unusual pattern to this year's epidemic, with a delayed start, and it isn't clear yet whether the peak has been reached santepubliquefrance.fr/maladies-et-tr… @SantePubliqueFr 7/n
what will happen in the UK?
very hard to predict & only a prospective study, collecting and releasing data in real time will allow us to see what is happening and act on this information
which is exactly what BronchStart @PERUKItweep sets out to do medrxiv.org/content/10.110… 8/n
very hard to predict & only a prospective study, collecting and releasing data in real time will allow us to see what is happening and act on this information
which is exactly what BronchStart @PERUKItweep sets out to do medrxiv.org/content/10.110… 8/n
some scenarios:
1. A larger unexposed cohort than usual with less maternal protection through recent RSV exposure, leads to larger peak than usual
2. Ongoing restrictions mean that we see a smaller peak, with rebound peak this autumn/winter when restrictions fully released 9/n
1. A larger unexposed cohort than usual with less maternal protection through recent RSV exposure, leads to larger peak than usual
2. Ongoing restrictions mean that we see a smaller peak, with rebound peak this autumn/winter when restrictions fully released 9/n
will RSV spread in its usual pattern (seeding through the metropolitan centres of London and Manchester thorax.bmj.com/content/75/3/2… @ThoraxBMJ ) or in a slower wave from France/Belgium northwards? 10/n

will we see an initial peak of rhinovirus bronchiolitis as restrictions are eased, followed by a delayed RSV peak? 11/n
all open questions, and in my opinion much more of a reason to worry about our summer holidays than vaccine passports
we need this information to understand how infants and children will present to EDs, guide decisions on palivizumab, and inform PICU service planning 12/n
we need this information to understand how infants and children will present to EDs, guide decisions on palivizumab, and inform PICU service planning 12/n
we welcome comments on the study pre-protocol medrxiv.org/content/10.110… & participation of your emergency department through the PERUKI network
we thank all the people who have contributed towards the design of this study so far 13/n
we thank all the people who have contributed towards the design of this study so far 13/n
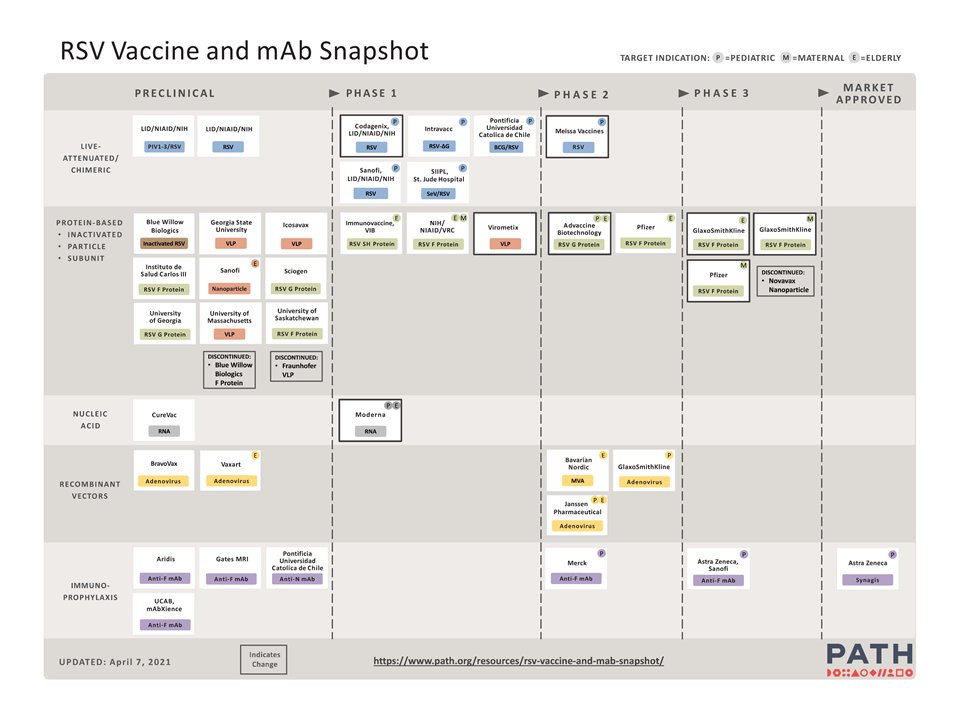
and hope that this study, and others like it, will contribute towards the introduction of an effective RSV vaccine path.org/resources/rsv-… END
• • •
Missing some Tweet in this thread? You can try to
force a refresh











