
With dozens of researchers at Yale, Stanford, Berkeley and IPA and several other organizations, we ran a cluster randomized trial involving almost 350,000 people and 600 villages in Bangladesh to assess the impact of community masking on COVID.
We conducted an intervention that increased mask-wearing by 29 percentage points using the techniques described here:
https://mobile.twitter.com/jabaluck/status/1392879291185119233?lang=en
With this 29 percentage point increase in mask-wearing, we saw a 9% drop in serologically confirmed COVID.
The reduction was larger in villages where we (randomly) used surgical masks than those where we used cloth masks; in surgical mask villages, we saw a 12% reduction in COVID overall and a 35% reduction among those aged 60+. 
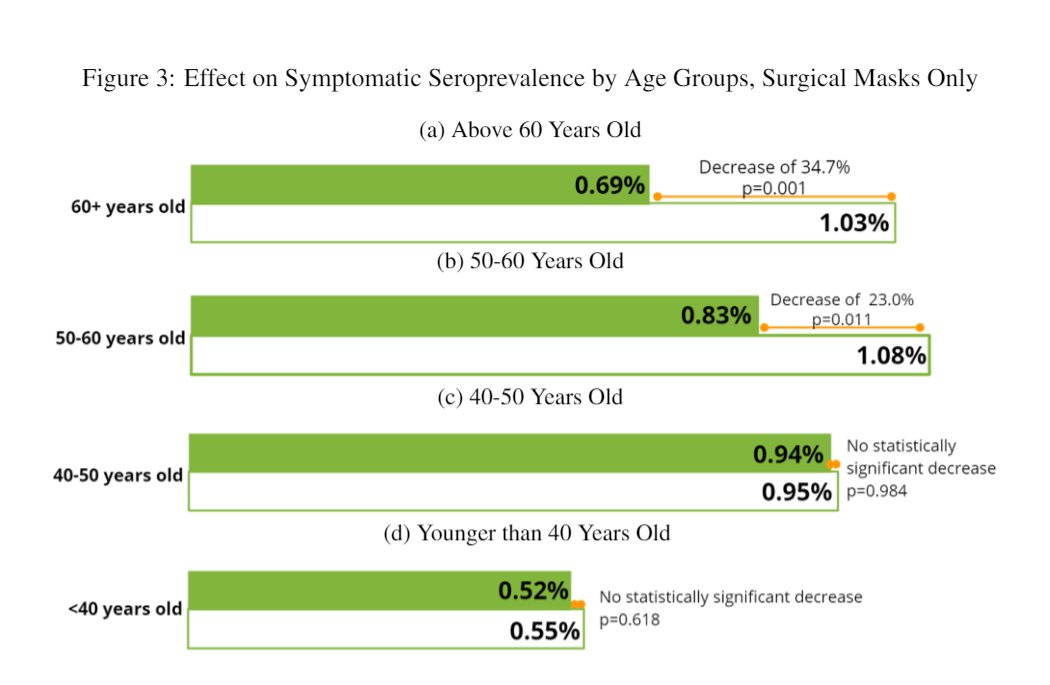
Since severe morbidity and mortality are concentrated among the elderly, this suggests that community-wide masking can be an extremely effective tool to combat COVID.
If going from 13/100 to 42/100 people wearing masks leads to reductions of the magnitudes above, near universal mask-wearing (as is possible with enforced mandates in some areas) might lead to substantially larger reductions.
As noted, we find especially convincing evidence that surgical masks are effective. Cloth masks reduce COVID symptoms, but the effect we find on symptomatic infections (confirmed via blood tests) is driven by surgical masks.
Cloth masks are likely better than nothing, but surgical masks or masks with higher filtration efficiency should be preferred to cloth masks where available.
A longer discussion of our intervention is available here, along with the underlying working paper: poverty-action.org/study/impact-m…
In subsequent posts, which I'll link here when available, I'll say more about how our study fits into the existing literature, as well as caveats and policy implications.
In the next few weeks, we'll post a public GitHub package with all of our data and analysis (with identifiers removed).
Some follow-ups: I should note that the PIs on this project were myself and @mushfiq_econ (economists at Yale), @Kwong_Laura, Steve Luby and Ashley Styczynski, epidemiologists and environmental scientists at Stanford (and in Laura's case, now Berkeley!).
The promised thread on how this fits into the existing literature is here:
https://twitter.com/Jabaluck/status/1433067145748000778
The promised policy / cost-benefit analysis thread is here:
https://twitter.com/Jabaluck/status/1433082245997232132
• • •
Missing some Tweet in this thread? You can try to
force a refresh


