
The Biden Administration declared this week to be #OverdoseAwarenessWeek.
And they did something absolutely unforgivable that will cost people their lives and freedom: They proposed extending the class-wide scheduling of fentanyls.
A thread 🧵
whitehouse.gov/ondcp/briefing…
And they did something absolutely unforgivable that will cost people their lives and freedom: They proposed extending the class-wide scheduling of fentanyls.
A thread 🧵
whitehouse.gov/ondcp/briefing…
1) Currently, fentanyl is a scheduled substance. Some analogues with proven high potency have been scheduled as Schedule 1.
Class-wide scheduling means that EVERY FENTANYL ANALOGUE EVER SEIZED IN THE FUTURE will be treated as a Schedule 1 drug with harsh penalties. Huge problem.
Class-wide scheduling means that EVERY FENTANYL ANALOGUE EVER SEIZED IN THE FUTURE will be treated as a Schedule 1 drug with harsh penalties. Huge problem.
2) Schedule 1 status means a drug has "high abuse potential" and "no medical use." It also means harsh penalties.
But not all fentanyl analogues are psychoactive or are potent. Some have no effects or milder effects than fentanyl. This incorrectly presumes analogue = dangerous.
But not all fentanyl analogues are psychoactive or are potent. Some have no effects or milder effects than fentanyl. This incorrectly presumes analogue = dangerous.
3) Before 2018, if a fentanyl analogue was seized, the burden would be placed upon the prosecution/State to prove that this analogue was highly potent or dangerous.
Then governments could use the EXISTING "Analogue Act" to prosecute people for it.
Then governments could use the EXISTING "Analogue Act" to prosecute people for it.
4) In some ways, the class-wide scheduling of fentanyl analogues is Drug War Theater- it makes it look like we're "doing something" about fentanyl. Even while there's already laws on the books at their disposal.
They just don't want to have to work to prove their cases.
They just don't want to have to work to prove their cases.
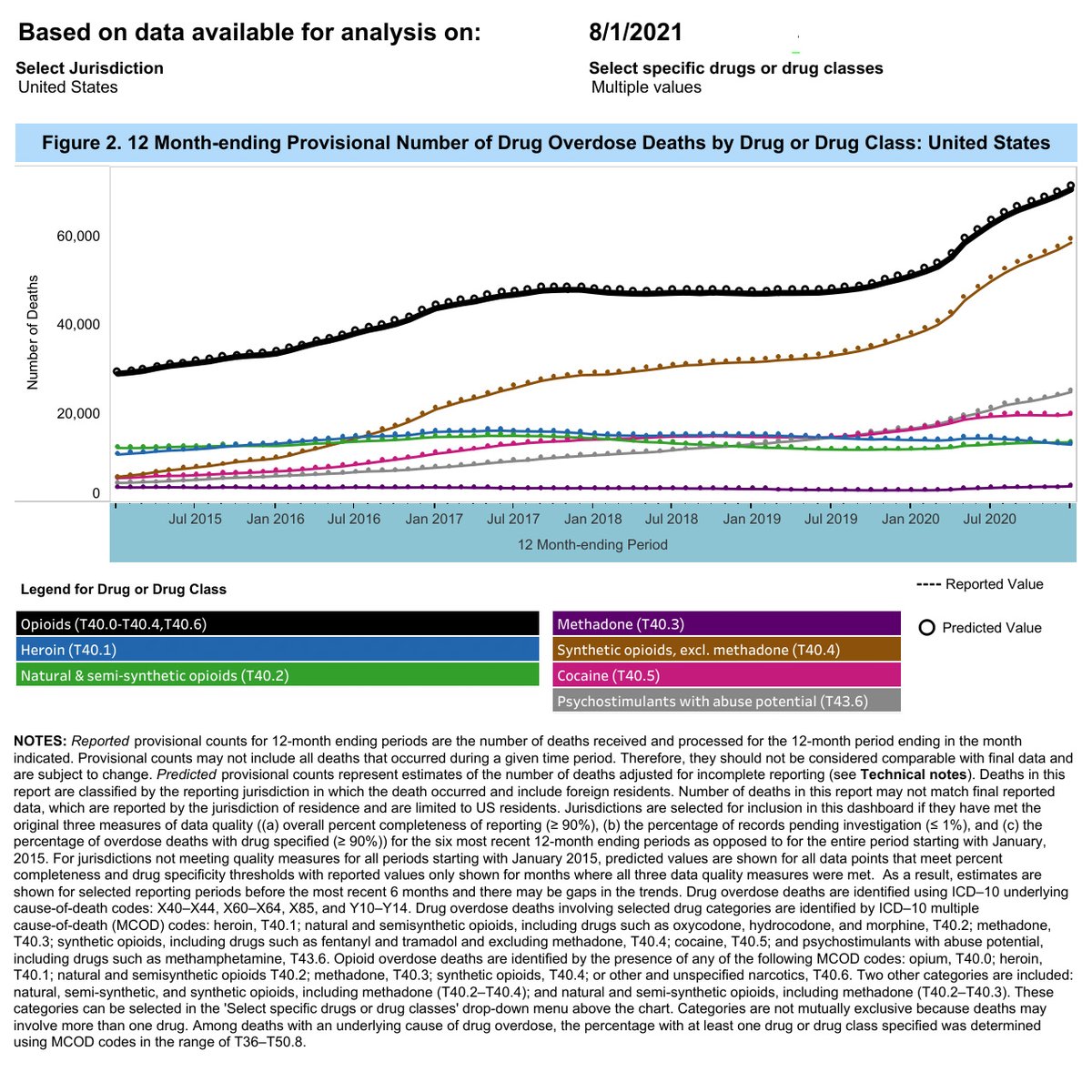
5) Also- we've temporarily had fentanyl class-wide scheduling since 2018. It's not working.
The brown line in the image below is "synthetic opioid" involved overdose deaths (including fentanyl and analogues). It has only increased. Nearly 2/3 of all deaths in 2020 had them.
The brown line in the image below is "synthetic opioid" involved overdose deaths (including fentanyl and analogues). It has only increased. Nearly 2/3 of all deaths in 2020 had them.
6) Check out US Sentencing Commission's own report about fentanyl analogue prosecutions.
(not sure why stock image is medicinal fentanyl while ODs are for illicitly manufactured fentanyls)
ussc.gov/research/resea…
(not sure why stock image is medicinal fentanyl while ODs are for illicitly manufactured fentanyls)
ussc.gov/research/resea…
7) Longer sentences, predominantly minority defendants, many did not know they had fentanyl/analogues, most were low level sellers.
Also- "any detectable amount" could trigger charges. If granules in a bag of heroin, you get penalties based on the full quantity of the heroin.
Also- "any detectable amount" could trigger charges. If granules in a bag of heroin, you get penalties based on the full quantity of the heroin.
8) This also places the burden on Health and Human Services to prove any fentanyl analogues are not potent/psychoactive so they can be removed from scheduling. And THEN they can go back and retroactively reduce expunge records of wrongfully convicted 🤬
9) This also has a negative impact on researchers who want to understand and study analogues. Scheduled drugs are hard to get approval to study. We could be missing out on the next MAT for OUD or pain treatment medication.
10) To learn more about each of these, you can tune into this conference we co-hosted back in March with expert panels discussing all of these challenges.
Speakers include me, @grantwilder3 @ptrisha80 @RyanMarino @DanCiccarone @MarilynMosbyEsq
facebook.com/watch/67372216…
Speakers include me, @grantwilder3 @ptrisha80 @RyanMarino @DanCiccarone @MarilynMosbyEsq
facebook.com/watch/67372216…
11) If this has infuriated you, PLEASE contact your Congresspeople. Temporary class-wide scheduling actually expires in October.
They can still let it expire.
Tell them to co-sponsor the STOP Fentanyl Act instead. FIN. baldwin.senate.gov/press-releases…
They can still let it expire.
Tell them to co-sponsor the STOP Fentanyl Act instead. FIN. baldwin.senate.gov/press-releases…
• • •
Missing some Tweet in this thread? You can try to
force a refresh









