I've not followed the employment tribunal case between Appleby and the Tavistock in great detail, but since they've concluded the process, it's time to have a read and see what they found.
This is a case about whistleblowing from within GIDS, specifically by one of the members on the Tavistock and Portman trust's Safeguarding team. About a dozen current and former staff were heard. Several thousand pages of relevant documents were gathered.
The "Findincs of Fact" are fairly straight forward, but also offer some insight into how these things can be handled. For example, the description of gender dysphoria does not fall for the usual sex/gender conflation trick, instead stating...
...that it results from "incongruence between a person's perceived gender identity and the gender assigned at birth or their biological sex" - a graceful way to handle the issue where activists try to equivocate between sex and gender in order to make sex non-factual.
They describe the nuances of the process quite well, highlighting how the vagueness of the diagnosis mean the treatment path that is being followed tends to be arbitrary and based on clinical judgement rather than an established model of care.
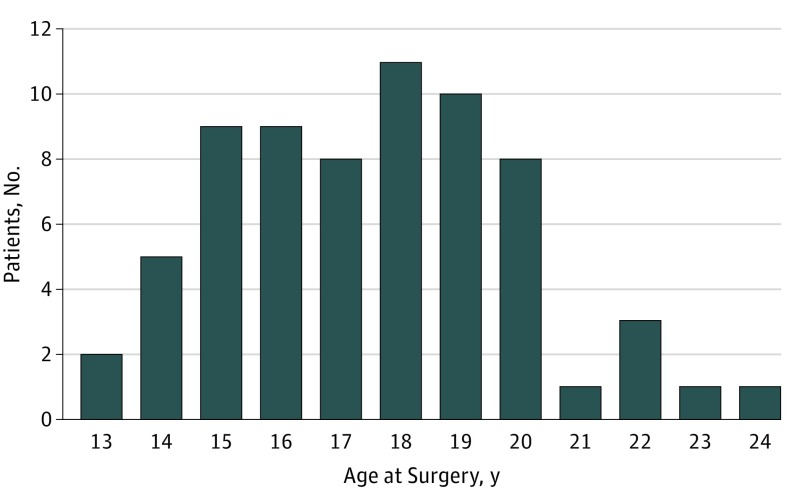
They describe the explosive growth (on Twitter usually just called "4400%") for this particular clinic as well as the sex ratio and overall demographic shift. Usually when someone brings this up, it means they already do not buy into the "it's just social acceptance" argument.
They also state "External pressure from campaigners (including a group called Mermaids) and some parents made difficult clinical decisions more difficult, and in consequence there were staff who sometimes found detachment difficult."
The claimant (Appleby) has worked as a social worker and children's guardian since the 1980's, employed by the Trust from 2004 onwards and is the named Safeguarding Lead for Children. She has quite the senior position, and is the person in charge of making sure the kids are safe.
In 2016 she reported to the Trust Board that "the increasing pressure of rising referral numbers had an impact that was distressing and even traumatic", noting "deficiencies in reporting on cases, in particular on Safeguarding"
During 2016 and 2017, a private GP (Dr. Webberley, of GenderGP fame) started issuing private prescriptions for puberty suppression to people currently being assessed by GIDS (!) or on their waiting list.
"Staff were uncertain how to deal with this."
"Staff were uncertain how to deal with this."
Appleby raised the issue with the medical director, Dr. Senior, who convened a meeting in June 2017 between Appleby and Dr. Carmichael, the Director of GIDS. There was an agreement that there needed to be someone at GIDS designated to link up with the central Safeguarding team.
The next part is quite interesting, I've attached the full part as an image, but it seems like the immediate concern from the director (Dr. Carmichael) was not to actually make use of this but to make sure it did not interfere with business as usual. 

They note that following this June 2017 development, there was a meeting between Mr. Richardson and two staff about "improving GIDS' understanding of Safeguarding", but in practice "little or nothing changed until March 2018."
Four months after the initial meeting, Appleby described the situation to Dr. Senior. At this point it's pretty explicit: staff is reporting a conflict between safeguarding and "transphobia", and it's becoming heated.
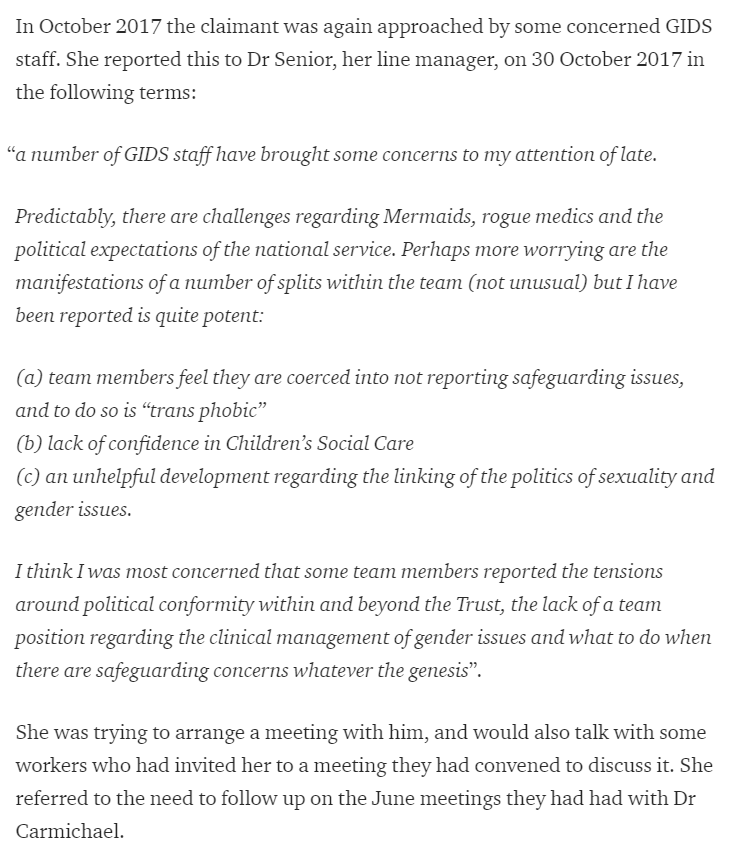
Two weeks later, she followed this up with a more detailed list of issues, including noting that there were concerns that suspended doctors were interfering, the explosive growth, and that even discussing issues like those was simply being ignored as "transphobic" by management.
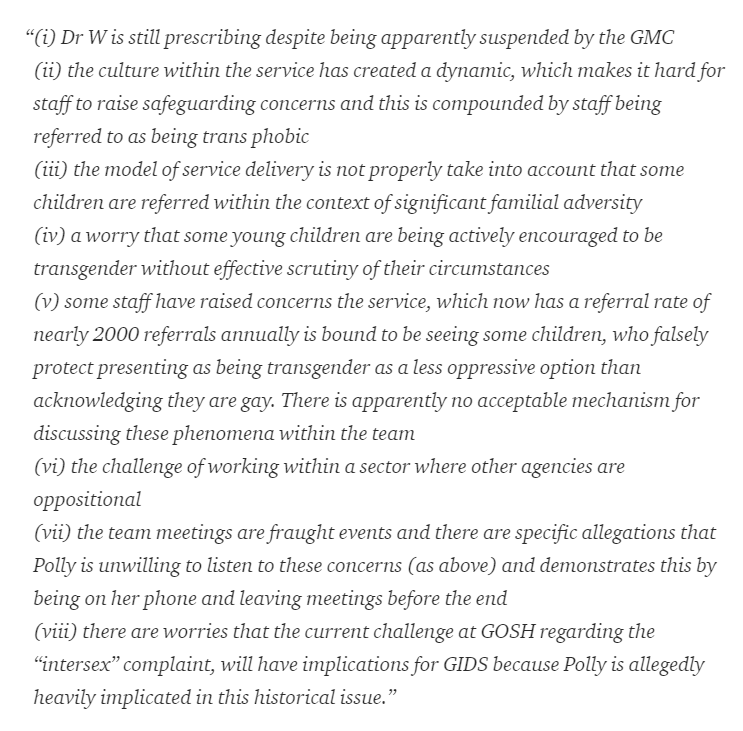
Appleby continued “I discussed some of these matters with you several weeks ago. You advised you would advise Sally" before noting that a fourth staff member had approached her with these concerns.
"Regrettably, Dr Senior did not advise, or reply at all."
"Regrettably, Dr Senior did not advise, or reply at all."
In January 2018 the Head of Social Work for the Tavistock emailed Appleby and Dr. Senior, with a copy to Mr. Richardson (the supposed local Safeguarding link in the GIDS), about a meeting of GIDS social workers and the need to "increase space for and dialogue about safeguarding".
Appleby replied to the email stating that she was already aware of "explicit concerns" which she had escalated twice and followed up on earlier in January. An email mixup ensues and Dr. Carmichael shows some signs of poor managerial behaviour, passive aggressive narcissism.
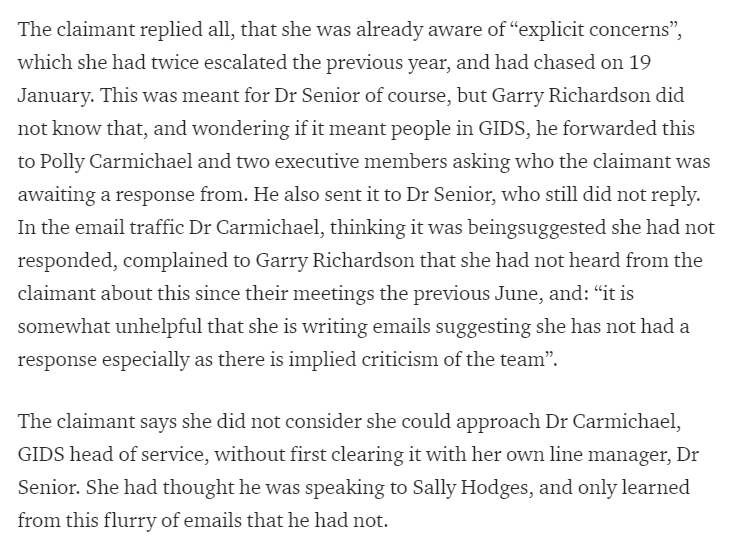
However, the first problem is identified: Dr. Senior hasn't done his job. On the 5th of February 2018, there is a meeting between Appleby and Dr. Carmichael where they get up to speed on what happened and a plan to move forward was set up.
Appleby was to talk to Mr. Richardson and Dr. Carmichael was to discuss it with her boss and her executive team, and the broken step of Dr. Senior would simply be bypassed in the future.
Interestingly there are three points under the header "Jimmy Savile". As background for those not familiar with the UK, this is a UK public figure (knighted as Sir James Savile) who also happened to be a massive child predator, something which was ignored during his...
...decades at the BBC, hosting children's shows. Although allegations trickled in steadily over the years, these were ignored and only after his death did the facade come crumbling down.
In a March 2018 meeting between Appleby and Mr. Richardson (now taking "an active role as safeguarding lead in GIDS") Appleby remarked that "if they were not careful a Jimmy Savile type situation could arise", however when Mr. Richardson expressed upset...
...she clarified that she did not mean that there was sexual abuse going on at GIDS but rather the risk of "an institution turning a blind eye to what was in front of them". "He did not discuss this remark with her further, then or later, but he was upset that she seemed to...
...think his professional colleagues in GIDS were aware children were not safe and wilfully ignoring it".
I'm not sure why this is relevant yet, but they also add that they note that Appleby used this phrase occasionally to describe the importance of vigilance in safeguarding.
I'm not sure why this is relevant yet, but they also add that they note that Appleby used this phrase occasionally to describe the importance of vigilance in safeguarding.
Moving on, "Early in 2018 ten concerned GIDS staff had also approach Dr David Bell, the staff representative on Trust's Board of Governors, and in April 2018 he and the claimant exchanged information about the concerns raised with each."
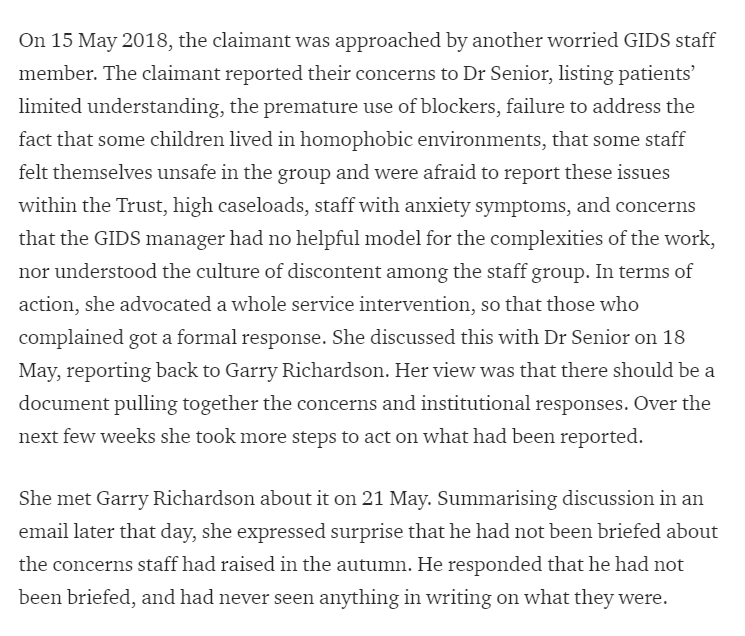
Apparently getting nowhere with Dr. Carmichael, as more staff came to her, Appleby apparently returned to Dr. Senior aiming to get a process written down on paper. Following this, she learned that Mr. Richardson had not been briefed on the prior issues.
Having seemingly correctly identified Dr. Senior, Dr. Carmichael and Mr. Richardson as unreliable at best, she instead reached out to Sally Hodges (this is the Director of Children, Young Adults and Families at the Tavistock Trust).
Noting that yet another GIDS worker (who she had not met before) had approached her with concerns about "children being given medication when they were unable to give informed consent, and when caseloads were very high. She reported the worker's concern about children...
...not having access to local mental health services, being exposed to abuse, that some may be gay, and that the challenges were not being thought about consistently."
She had a couple of meetings with Sally Hodges, who state that "the Trust management group had discussed it, and hoped to develop a clear action plan, and she asked the claimant for more detail." In the process of digging up more details, Appleby found that...
...the safeguarding systems for GIDS were wildly inadequate in all sorts of ways, as documented in the judgement.
This thread is already getting unmanageably long, so I'll be a bit briefer. I'm only halfway through this document!
This thread is already getting unmanageably long, so I'll be a bit briefer. I'm only halfway through this document!
Part of what she looked at was numbers: "in the entire service in 2017 there had been one record of safeguarding supervision, and only 11 recorded case discussions" - this is in light of the service seeing hundreds if not thousands of extremely complex cases.
"All this was now in the context of an impending CQC inspection. Polly Carmichael then cancelled the meeting with Garry Richardson about safeguarding reporting. She said she was on leave and wanted to be involved, at which the claimant protested that it was arranged...
...to discuss gaps in reporting, and had been supported by Sally Hodges. The meeting did then go ahead [...] and concluded that the claimant and Garry Richardson should continue to meet to discuss informatics."
Having the director of GIDS try to shut down safeguarding meetings that were "blessed" by her superiors is really quite interesting.
"The relationship between the claimant and Dr Carmichael and Garry Richardson was strained, as shown by the claimant having to explain in detail to Dr Carmichael, who had challenged her about it, why she had spoken directly to a...
...Cambridgeshire Designated Nurse about Safeguarding in a GIDS case."
Dr. Carmichael is really not coming out smelling of roses so far. Shutting down safeguarding and refusing to let others do it.
Dr. Carmichael is really not coming out smelling of roses so far. Shutting down safeguarding and refusing to let others do it.
Enter, stage left, the Bell report.
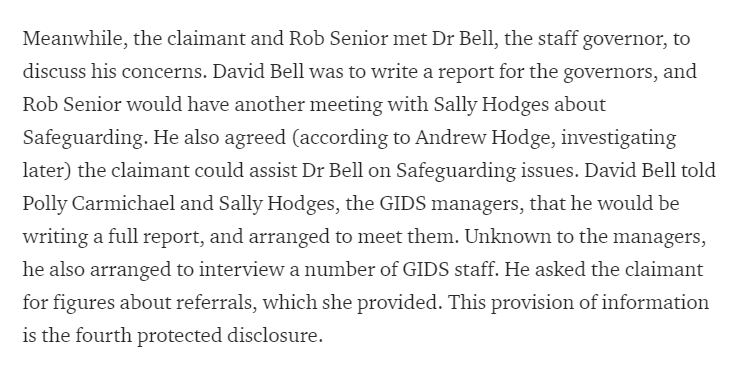
There are a few paragraphs about the Bell report including whether the report overstated Appleby's involvement with it, and that this might have "led colleagues to suppose that she adopted his views."
It continues "Dr Carmichael was certainly troubled by its 'divisive tone'. In her view the Bell report was 'not constructive or balanced'. More than that, she felt deceived that Dr Bell had interviewed her staff 'in guise of taking an interest', and then written a hatchet job."
In March 2018 Dr. Senior announced his retirement, and was replaced as Medical Director by Dr. Sinha, who was new to the Trust. As a newcomer he was commissioned to conduct a review of GIDS, which he started in October, interviewing 31 staff members.
Dr. Sinha describes Appleby as a bit of an asshole, including disliking her summaries of meetings (which she routinely asks people to confirm whether they are accurate) although he does not seem to have had much to do with her before forming this opinion.

Dr. Sinha then decides to waste everyone's time, something they enthusiastically agree to do, by treating Appleby as a leak who must be compartmentalized, suggesting that they are well aware that sunlight is a direct threat to them.

We're still in the handover phase, that's why Dr. Senior is still hanging around, looking to throw further wrenches into the gear. After not responding to prior issues for months he now gets back in less than an hour.
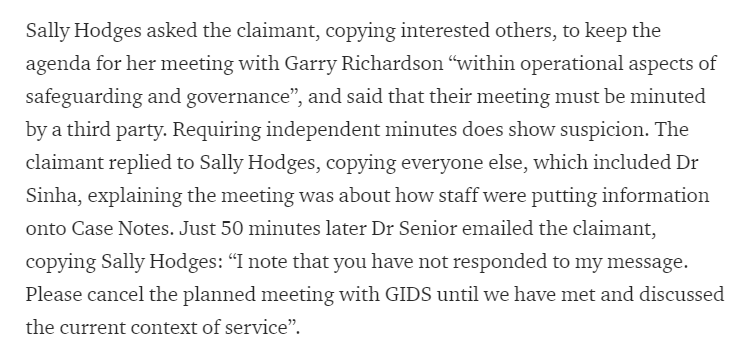
"He explained to the tribunal that he regarded it as insubordination that she had not replied directly to his unquiry on why she wanted the information, and that this was an example of her autonomous working, which he wanted to rein back."
The tribunal sees straight through him, noting "We were surprised: he had a detailed answer in the message to Sally Hodges, copied to him. The charitable view is that he not actually read the message to Sally Hodes."
"If he had read it, then he comes across as petulant. Moreover, if he did think she had an attitude problem, it might have been better to discuss it face-to-face rather than issue an order about not meeting a Safeguarding colleague about getting accurate statistics."
In late October 2018 Appleby was interviewed by Dr. Sinha as part of his GIDS review. She prepared a written statement, with appendicies. One of these were the recent exit interview with Matt Bristow (the fifth protected disclosure).
"The text is extensive, but incudes that there was homophobia in GIDS, that staff worked in a 'climate of fear', and referral outside the service (such as a Safeguarding report) was the last resort."
"When she handed the statement to Dr Sinha at the start of the meeting, he handed it unread to the note taker, and proceeded with his set questions."
He sounds quite incompetent.
He sounds quite incompetent.
"After the interview Dr Sinha emailed tersely instructing her not to interrogate any service for additional data or information without discussing it with him first, nor to take part in the ongoing board review of the GIDS service...
...and to have no contact with David Bell except with respect his clinical practice."
Actually, he sounds malicious.
Actually, he sounds malicious.
"In the spring of 2019 Dr Sinha presented his review report to the board. It was published in March 2019 with an action plan. This included having a Safeguarding lead within each division, as GIDS already did in Garry Richardson."
But what if the lead isn't doing their job?
But what if the lead isn't doing their job?
Oh, I see, the Savile remark was regarding the first detriments, where taking this out of context was used to smear Appleby.
There's then some notes about Dr. Sinha being extremely petty surrounding unplanned major surgery for Appleby, and her sick leave being delayed due to wound infections.
The judgement notes "It is worth mentioning that the way this was handled reflects Dr Sinha's unsympathetic, almost hostile, relationship with the claimant."
They're not mincing words about it.
They're not mincing words about it.
Dr. Sinha went on to be extremely litigious about the thing, apparently going to HR about Mr. Richardson being emotionally upset about the Savile comment, "ambushing" Appleby with this by inviting her to "an informal meeting to discuss recent events regarding the GIDS".
She "emailed an account of the meeting to her union representative, emphasising that it was scheduled as an informal meeting, with no notice of the topic, or mention of bringing a companion [the HR rep], but the outcome was as if it was the conclusion of a disciplinary process."
Dr. Sinha stated "I further suggested that you should ensure you are mindful of any further statements made in the future in relation to this matter or any other that may cause offence to other colleagues."
What an incredibly petty man.
What an incredibly petty man.
To the tribunal he stated "finally, I confirmed that although this matter will not be taken further, this meeting will be documented and remain on your file. I may need to investigate the matter formally, if there are further reports of this type of incident".
This caused Appleby to lodge a grievance and present the claim to the tribunal. The Trust's HR department brought in an independent investigator who concluded that "Trust clinicians were divided between those who considered the Bell report an overreaction to the inherent...
...complexity of GIDS work, and those concerned about the increase in natal females identifying as male, that gender identity may be a proxy for same-sex orientation, and that there is no thorough exploration of the issues."
The investigator also concluded that "most saw the claimant as a concerned professional, not someone out to make trouble."
The second group of detriments are quite interesting, this is the overall claim being considered.

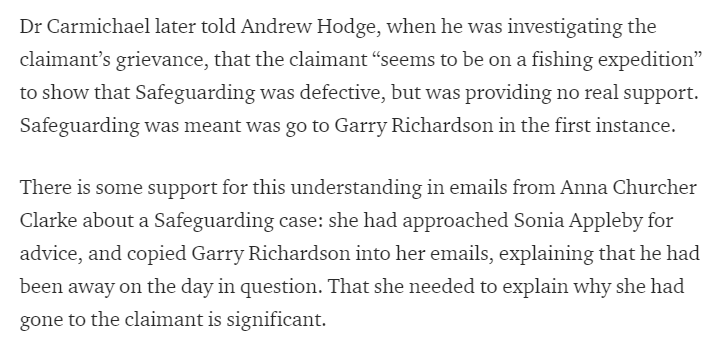
They note: "Nothing was ever put in writing to GIDS staff about reporting or not Safeguarding concern. In fact they were not even told in writing that Garry Richardson was the Safeguarding lead within GIDS, so the lack of writing does not mean of itself that this was not said."
They consider a number of statements surrounding this, which paint a pretty damning picture of the situation.

Spiladis describes further damning events.

Even in cases where domestic violence and emotional abuse is a concern, you should keep it all under wraps.
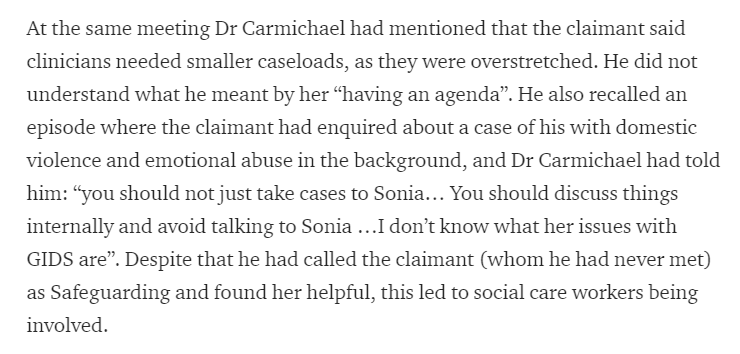
Most of this is based on a handful of clinicians statements, but they do note cracks in the culture of silence hint at what was really going on.
The judgement then summarizes everything prior over the next page and a half, with certain key points.
"Whether Dr Carmichael’s message to staff was being understood or misunderstood by them is hard to say, because nothing was ever put in writing, and both in emails, and in answers to questions in the tribunal, Dr Carmichael was often both verbose and imprecise."
They conclude that "there was a message being communicated to GIDS staff by Dr Carmichael, at the time of the Sinha review, that they should not take Safeguarding issues to the claimant, not because she was not a...
...clinician familiar with the complexities but because she was hostile to GIDS. What had been said in the December 2018 team meeting went beyond a mere statement of Safeguarding protocol."
"It was clear from Dr Carmichael's discussion after the event with [the independent investigator] that she did doubt the claimant's good faith and neutrality in what GIDS were doing."
This "lends credence to the perception of those working in the team that they were being told that the claimant was to be regarded as hostile to their work."
The language regarding Mr. Richardson does not hold and punches: "It was plain that Garry Richardson himself resented the claimant, as far back as September 2017".
"It is less clear how this impacted on the claimant herself, whose communication with others is notable as always scrupulously correct, andw ho stepping carefully, no doubt aware of the difficult politics and boundaries of expertise."
Mr. Richardson "told [the independent investigator] that he was more likely to go to Caroline McKenna for support and to discuss Safeguarding than to the claimant. This is surprising, as she is the adult Safeguarding lead."
Odd thing to confess: "I don't do my job."
Odd thing to confess: "I don't do my job."
"One result of these proceedings is that since they began the claimant and Garry Richardson have had little contact on Safeguarding at all."
And GIDS management did not seek to fix this failure of safeguarding.
And GIDS management did not seek to fix this failure of safeguarding.
Following that, there are a couple of pages of legal consideration which are interesting but not worth repeating on Twitter, I would encourage everyone to read the actual judgement.
In their discussion, they reason that the enforced third party minutes, the ambush and thinly veiled threat were detriments. I would tend to agree, and they state that they find it reasonable to consider these as unlabeled disciplinary acts.
"Further, there was no investigation. Had there been, Dr Sinha would have learned that this was indeed part of her standard training presentation"
Overall they're quite scathing of his professional incompetence.
Overall they're quite scathing of his professional incompetence.
They state that Dr. Sinha did nothing to mend relationships, and that "He was judgemental and punitive; he believed Garry Richardson and not her."
The tribunal appears unsatisfied with his excuse for this, as it does not seem accurate.
The tribunal appears unsatisfied with his excuse for this, as it does not seem accurate.

They continue: "We found it hard to credit that the only reason Dr Sinha treated her in this way was because he thought she was resistant to line management and needed to be brought into line. By July 2019 extensive press coverage of the matters she had raised, given...
...the leaking Dr Bell’s report, had contributed to a febrile ‘them and us’ mentality."
In other words an inability to maintain a professional standard. This is unacceptable for such a high profile clinic as the GIDS, where children are treated.
In other words an inability to maintain a professional standard. This is unacceptable for such a high profile clinic as the GIDS, where children are treated.
"Dr Sinha’s quasi-disciplinary treatment of her can only be explained as materially influenced by her disclosures, which were viewed by him (and others) as unwarranted interference, overstepping her proper role."
As for the secondary detriments, in terms of reputation and professional standing, they state "We do not consider that the making of disclosures about GIDS work and Safeguarding can be severed from the way the claimant handled...
...the information. She was subjected to the second group of detriments because she made them."
In other words, she was treated as shit because she blew the whistle.
In other words, she was treated as shit because she blew the whistle.
As a last gasp defence, "the respondent argues that the addition of the second group of detriments was out of time, and that it came to the claimant's attention much earlier, perhaps as much as a year before the amendments in February or Match 2020"
This is essentially "you got us, but what about the statute of limitations?" for which the tribunal says that Appleby learned of these gradually, and that "when the documents were disclosed, she amended in a reasonable time therafter."
So, what is the ruling on this tribunal case? For Appleby, and the primary and secondary detriments, the tribunal states "the award is £20,000" and that "Both senses of injury are likely to resolve on receipt of this judgment vindicating her position."
For the Tavistock and Portman Trust, the GIDS, it's just another blight on their already dreadful record. The organization appears rotten to the core and unable to mend itself.
For Dr. Carmichael? For Dr. Sinha? For Mr. Richardson? It's their dirty laundry aired out in public, and their names tarred by their own actions. They appear to be petty and pathetic people.
Will they suffer professionally? Not as long as the Tavistock doesn't change course.
Will they suffer professionally? Not as long as the Tavistock doesn't change course.
• • •
Missing some Tweet in this thread? You can try to
force a refresh