This preprint looking at the risk of vaccine-related side-effects vs COVID-19 infections for children has received a lot of attention, and people have been asking my opinions on it. So, a few thoughts 1/n
https://twitter.com/TracyBethHoeg/status/1435796377188003841
2/n The preprint itself is pretty simple - comparing the calculated risk per million vaccines of having a VAERS report consistent with myo/pericarditis (CAE) with the number of COVID hospitalizations per 100,000 children aged 12-17 

3/n The authors found that the rate of VAERS reports consistent with myocarditis was higher than the average rate of COVID hospitalizations per 100,000 children in a population where there was a reasonably high current prevalence of COVID-19

4/n To think about this, it's important to note what VAERS is - it is a passive reporting system (the acronym stands for Vaccine Adverse Event Reporting System) that anyone can enter in a report to cdc.gov/vaccinesafety/…

5/n Because this system is designed to be sensitive and pick up even quite rare harms, there are some caveats, most notably that (as the CDC points out) you cannot determine whether a vaccine caused a specific issue from VAERS alone

6/n So I'm a bit confused by the terminology here. As far as I can see, the authors have relied entirely on VAERS to determine case figures, which the sources they reference point out cannot be considered a causal link
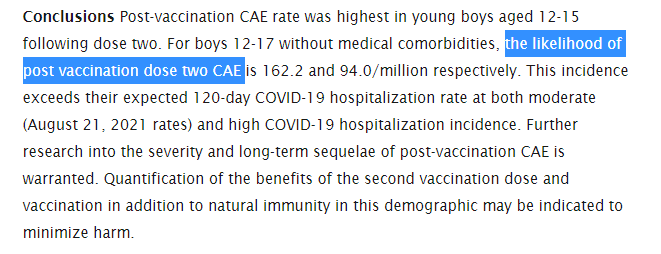
7/n In other words, it's not the likelihood of experiencing a post-vaccination CAE, but the likelihood of having a post-vaccination REPORT of a CAE per million children
8/n This may sound like needless pedantry, but it isn't - media reporting and attention are a known confounder of passive reporting systems like VAERS. If you have a lot of news articles, you get more reports, even if those are not actually linked to the vaccines

9/n And it's interesting to note that, as the authors point out, the CDC (who use much more detailed information to calculate these rates) have a lower estimate of post-vaccine CAE than this preprint

10/n The second point that confuses me about the paper as it currently stands is comparing two numbers with very different denominators:
1. events per 1mil vaccines
2. events per 1mil children per 120 days
1. events per 1mil vaccines
2. events per 1mil children per 120 days

11/n One way to think about this disparity is to simply equalize the denominators. We could do this by calculating the 120-day risk of CAE following vaccination for males aged 16-17 in the United States

12/n Based on the numbers in table 1, that would be 110 total events (doses 1+2), and a population of about 3 million, so very crudely 37 CAEs per 120 days
This is lower than most of the calculated rates of COVID-19 related admissions in the paper
This is lower than most of the calculated rates of COVID-19 related admissions in the paper

13/n Alternatively, we could compare the risk having a CAE after vaccination with the risk of hospitalization for kids per INFECTION
Fortunately, there's already a great resource for doing this in a recent preprint medrxiv.org/content/10.110…
Fortunately, there's already a great resource for doing this in a recent preprint medrxiv.org/content/10.110…

14/n From this preprint, the likelihood that a child aged 16-17 will experience an infection severe enough to warrant hospitalization is about 1 in 500, and the risk of needing ICU is about 1 in 4,000
15/n So might reasonably compare the risk of 94-168 CAEs per million vaccinations posited by this paper with the risk of 2,400 hospitalizations expected per million infections with COVID-19
16/n Now, it is worth noting that this assumes that the risk of eventually contracting COVID-19 is 100% for children who are not vaccinated, however as time moves on that is not, I think, entirely unreasonable
17/n I think weighing the competing risks of vaccination vs infection is a very challenging thing to do, so I commend the authors on the preprint. I think these might be things to consider when updating it for future versions
18/n That being said, I'm not sure I agree that this preprint shows vaccination to be riskier than immunization for these age groups/genders. Not an easy question to answer!
19/n This piece from @dfreedman7 is a fairly startling addition to the discussion. The implication appears to be that even the basic case definition the authors used was entirely useless, which is less than ideal
https://twitter.com/dfreedman7/status/1437229791380443139?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh