
1/ 🧵
Time for a #tweetorial on simple #ECG interpretation
When I learned to read ECGs, my biggest fear was to miss an important finding!
To avoid that: Be systematic❗️
My simple approach to ECGs with 8 steps 🪜👇
#medicalstudent #education #cardiotwitter #medtwitter #EPeeps
Time for a #tweetorial on simple #ECG interpretation
When I learned to read ECGs, my biggest fear was to miss an important finding!
To avoid that: Be systematic❗️
My simple approach to ECGs with 8 steps 🪜👇
#medicalstudent #education #cardiotwitter #medtwitter #EPeeps
2/
‼️ All following ECGs are with paper speed of 25 mm/s and a signal gain of 10 mm/mV ‼️
Therefore:
1 small square = 40 ms
1 big square = 200 ms
Now we are ready to read the ECG systematically
‼️ All following ECGs are with paper speed of 25 mm/s and a signal gain of 10 mm/mV ‼️
Therefore:
1 small square = 40 ms
1 big square = 200 ms
Now we are ready to read the ECG systematically

3/
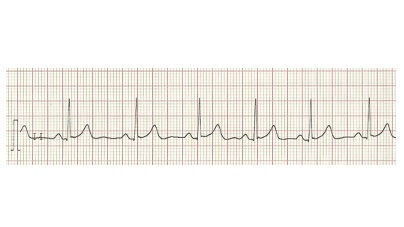
1⃣ Rhythm
Sinus rhythm or abnormal rhythm?
(Also note if regular or irregular)
Normal: One P-wave precedes each QRS complex (sinus rhythm)
Interpret from the lead that shows the P-wave most clearly (usually lead II)
1⃣ Rhythm
Sinus rhythm or abnormal rhythm?
(Also note if regular or irregular)
Normal: One P-wave precedes each QRS complex (sinus rhythm)
Interpret from the lead that shows the P-wave most clearly (usually lead II)

4/
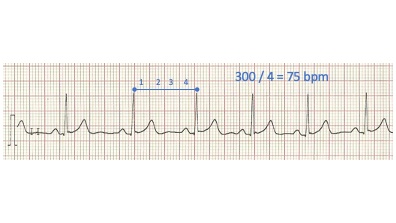
2⃣ Frequency
Regular rhythm: 300 divided by number of big squares between QRS complexes
Irregular rhythm: Number of QRS complexes per 3s multiplied by 20
Assess both atrial and ventricular frequency if dissimilar
2⃣ Frequency
Regular rhythm: 300 divided by number of big squares between QRS complexes
Irregular rhythm: Number of QRS complexes per 3s multiplied by 20
Assess both atrial and ventricular frequency if dissimilar
5/
3⃣ P-wave morphology
👉 assess the width and height
Normal: ≤3 mm wide and ≤3 mm tall
>3 mm tall ➡️ enlargement of the RA (P-pulmonale?)
>3 mm wide ➡️ enlargement of the LA (P-mitrale?)
3⃣ P-wave morphology
👉 assess the width and height
Normal: ≤3 mm wide and ≤3 mm tall
>3 mm tall ➡️ enlargement of the RA (P-pulmonale?)
>3 mm wide ➡️ enlargement of the LA (P-mitrale?)

6/
4⃣ PR interval
👉 assess the length
Normal: 120-220 ms
If abnormal, AV-block may be present
Check out the tweetorial about AV node physiology by @AvrahamCooperMD here: bit.ly/3CbBZg0
4⃣ PR interval
👉 assess the length
Normal: 120-220 ms
If abnormal, AV-block may be present
Check out the tweetorial about AV node physiology by @AvrahamCooperMD here: bit.ly/3CbBZg0

7/
5⃣ QRS complex
👉assess the width, axis, amplitude and Q-waves
Let's take them one by one 👇
5⃣ QRS complex
👉assess the width, axis, amplitude and Q-waves
Let's take them one by one 👇

8/
Length of the QRS complex
Normal: ≤120 ms
If >120 ms, several causes exist: LBBB/RBBB, ventricular arrhythmia, pre-excitation, ventricular pacing, aberrant conduction, PVCs, electrolyte derangement etc.
Length of the QRS complex
Normal: ≤120 ms
If >120 ms, several causes exist: LBBB/RBBB, ventricular arrhythmia, pre-excitation, ventricular pacing, aberrant conduction, PVCs, electrolyte derangement etc.

9/
Axis: Fast and simple approach: Look at lead I and aVF:
Normal: Positive QRS in I and aVF
Left⏪: Positive QRS in I, negative in aVF
Right⏩: Negative QRS in I, positive in aVF
Axis: Fast and simple approach: Look at lead I and aVF:
Normal: Positive QRS in I and aVF
Left⏪: Positive QRS in I, negative in aVF
Right⏩: Negative QRS in I, positive in aVF

10/
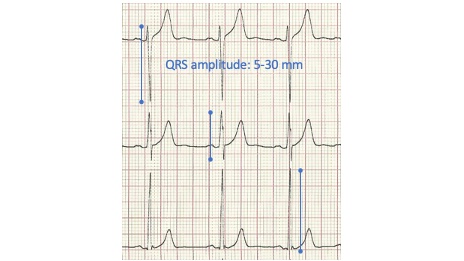
Amplitude of the QRS complex
Normal: 5-30 mm (rule of thumb – several criteria exist)
>30 mm: May be due to ventricular hypertrophy
<5 mm (low voltage): May be due to pericardial effusion, hyperthyroidism, obesity etc.
Amplitude of the QRS complex
Normal: 5-30 mm (rule of thumb – several criteria exist)
>30 mm: May be due to ventricular hypertrophy
<5 mm (low voltage): May be due to pericardial effusion, hyperthyroidism, obesity etc.
11/
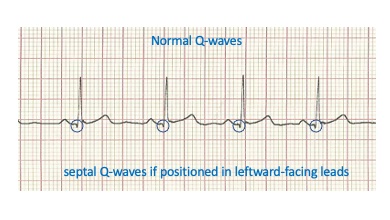
Q-waves present?
Normal: <1 mm wide and <2 mm deep
If wider/deeper: Pathological – may be due to necrotic tissue (electrically dead) and the lead therefore record a current running from endocardium to epicardium in the opposite myocardial wall (➡️ negative deflection)
Q-waves present?
Normal: <1 mm wide and <2 mm deep
If wider/deeper: Pathological – may be due to necrotic tissue (electrically dead) and the lead therefore record a current running from endocardium to epicardium in the opposite myocardial wall (➡️ negative deflection)
12/
6⃣ ST segment
👉 deviations from the J-point?
Normal: Isoelectric
>1 mm elevation (except in V2-3, elevation should be higher): May be #STEMI
>0.5 mm depression: May be #NSTEMI
Note, deviations may also be due to several other conditions than #AMI‼️
6⃣ ST segment
👉 deviations from the J-point?
Normal: Isoelectric
>1 mm elevation (except in V2-3, elevation should be higher): May be #STEMI
>0.5 mm depression: May be #NSTEMI
Note, deviations may also be due to several other conditions than #AMI‼️

13/
7⃣ T-wave morphology
👉assess deflection, symmetry and height
Normal: Upright in all leads except aVR and V1, asymmetric, <5mm in limb leads and <10mm in precordial leads
If abnormal: Ischemia, electrolyte derangement, structural heart disease, PE etc. may be considered!
7⃣ T-wave morphology
👉assess deflection, symmetry and height
Normal: Upright in all leads except aVR and V1, asymmetric, <5mm in limb leads and <10mm in precordial leads
If abnormal: Ischemia, electrolyte derangement, structural heart disease, PE etc. may be considered!

14/
8⃣ QT interval
👉assess the length
Rule of thumb: Normal QT is less than half the preceding RR interval
However, QTc are more precise and may be applied
QTc is prolonged if >440ms in 👨 or >460ms in 👩 and shortened if <350ms
QTc >500 ms ➡️ increased risk of TdP
8⃣ QT interval
👉assess the length
Rule of thumb: Normal QT is less than half the preceding RR interval
However, QTc are more precise and may be applied
QTc is prolonged if >440ms in 👨 or >460ms in 👩 and shortened if <350ms
QTc >500 ms ➡️ increased risk of TdP

15/
💥Summary💥
Be systematic and use the 8 simple steps 🪜
Once you have seen multiple normal ECGs it may be easier to spot an abnormality
If you are in doubt 👉 seek expert help as even minor ECG abnormalities may be due to severe pathology
💥Summary💥
Be systematic and use the 8 simple steps 🪜
Once you have seen multiple normal ECGs it may be easier to spot an abnormality
If you are in doubt 👉 seek expert help as even minor ECG abnormalities may be due to severe pathology

16/
Thank you for reading the #tweetorial
Please re-tweet, like, and tag peers who may find it useful 🙏
@EmilHolckMD @TanjaCharlotteF @arnelasaljic @Dominik_Linz @ThomasJesperse6 @DCAcademyDK @AUHCardio @MedTweetorials
Thank you for reading the #tweetorial
Please re-tweet, like, and tag peers who may find it useful 🙏
@EmilHolckMD @TanjaCharlotteF @arnelasaljic @Dominik_Linz @ThomasJesperse6 @DCAcademyDK @AUHCardio @MedTweetorials
• • •
Missing some Tweet in this thread? You can try to
force a refresh



