
1/6. This chart shows you everything you need to know about localizing foot drop. But let’s make it even simpler. If dorsiflexion is weak, there is one muscle that really matters: the tibialis posterior, which does ankle INVERSION. Let’s unpack that with a cool mnemonic. 
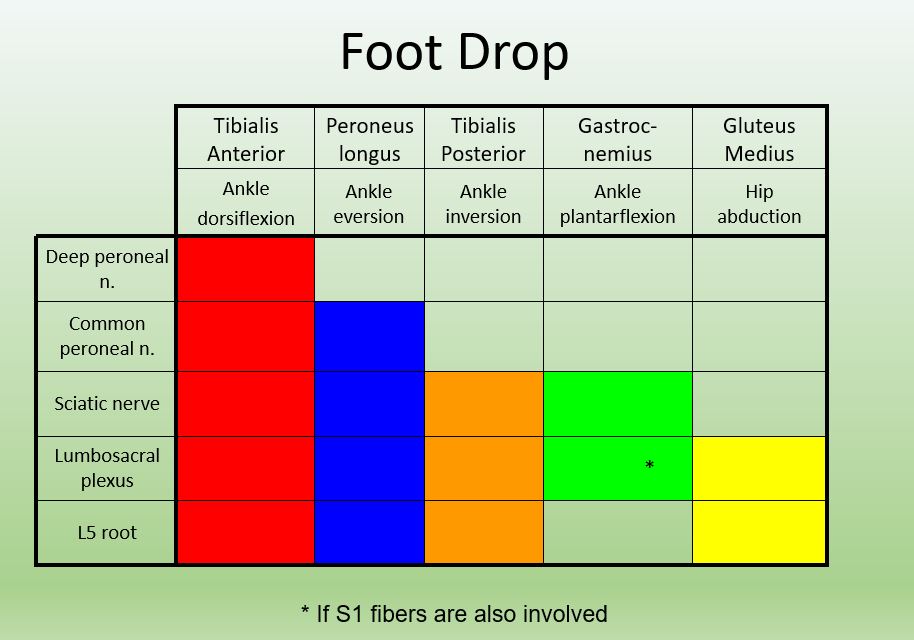
2/6 Common things are common, and most of the time, a foot drop is caused by either:
- A common peroneal neuropathy at the fibular head or
- An L5 radiculopathy.
- A common peroneal neuropathy at the fibular head or
- An L5 radiculopathy.
3/6. The peroneal nerve (which we already know is responsible for dorsiflexion) has two E’s in it. That should remind you that the PERONEAL nerve is responsible for EVERSION, through supplying the peroneus longus.

4/6. The TIBIAL nerve has two I’s in it, and I is for Inversion. The tibial nerve supplies the tibialis posterior, which inverts the ankle. (But not the tibialis anterior, which does dorsiflexion. A tibial neuropathy isn't going to cause foot drop.)

5/6. If you write it out, L-FIVE has both an I and an E. That should remind you that L5 supplies both ankle INVERSION and ankle EVERSION. Both the tibialis posterior and the peroneus longus are mostly L5-innervated.

6/6. So if L5 supplies both inversion and eversion, and the peroneal nerve only supplies eversion, what action can be used to distinguish them?
INVERSION.
Foot drop with inversion weakness is from an L5 lesion, and foot drop without inversion weakness is more likely peroneal.
INVERSION.
Foot drop with inversion weakness is from an L5 lesion, and foot drop without inversion weakness is more likely peroneal.
Let me know what you think! @Inside_TheMatch , @aanmember, @nmatch2022,
#neurology, #futureneurologist, #neurotwitter, #neurotwitternetwork, #tweetorial @AANEMorg #neuromuscular
#neurology, #futureneurologist, #neurotwitter, #neurotwitternetwork, #tweetorial @AANEMorg #neuromuscular
• • •
Missing some Tweet in this thread? You can try to
force a refresh


