MMWR AZ 🌵 mask study #1 limitation:
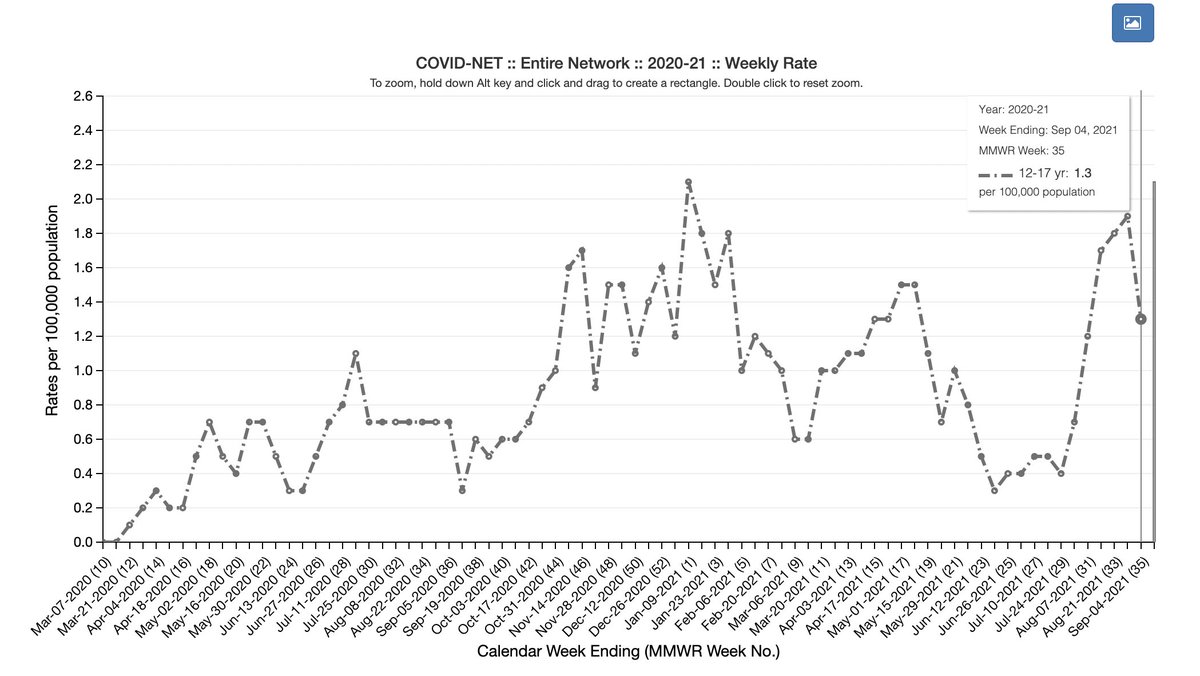
-Not adjusting for community cases in Maricopa Co (R) rising more during the study (see Figures)
-They adjusted for pre-study case rates, but that was not enough
-remember ~ 95% of school cases come from the community!
cdc.gov/mmwr/volumes/7…
-Not adjusting for community cases in Maricopa Co (R) rising more during the study (see Figures)
-They adjusted for pre-study case rates, but that was not enough
-remember ~ 95% of school cases come from the community!
cdc.gov/mmwr/volumes/7…

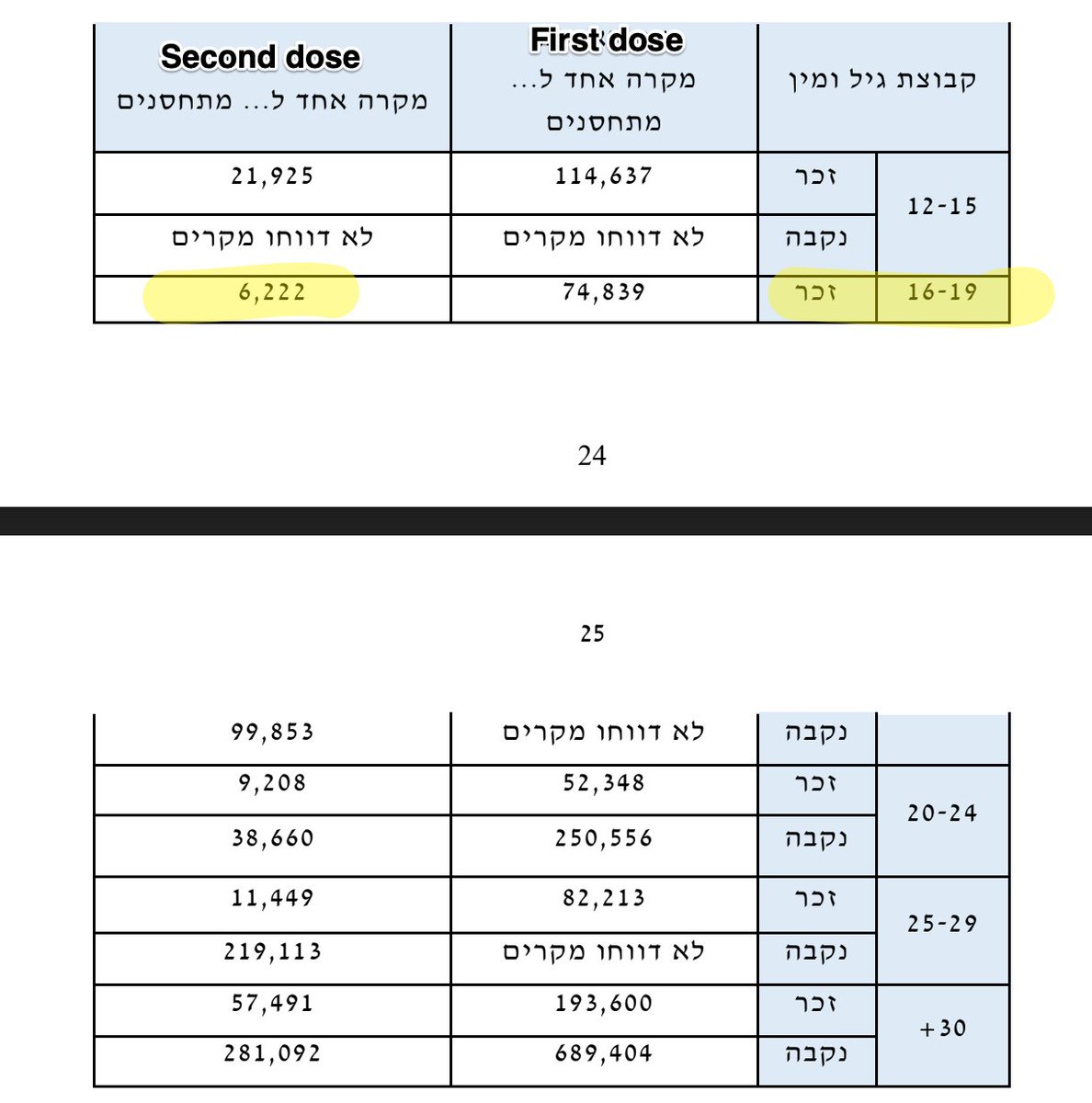
Maricopa also had a lower vaccination rates: 47.6% vs 59.2% in Pima.
Likely the entire story here is more school cases in schools w/o mask mandates (mostly in Maricopa) due to higher comm. case rates related to lower vax rates. How did this become a mask story?🤔
Likely the entire story here is more school cases in schools w/o mask mandates (mostly in Maricopa) due to higher comm. case rates related to lower vax rates. How did this become a mask story?🤔
Since I am literally sitting on the side of a soccer field in Stockton, for further info, I want to refer you to @VPrasadMDMPH 's discussion of these two MMWR studies & why we unfortunately can't learn about the effectiveness of masks from them. vinayprasadmdmph.substack.com/p/two-new-cdc-…
Here were my main critiques of the other (Budzyn et al) mask study in MMWR ⬇️
https://twitter.com/TracyBethHoeg/status/1441575701316988936
• • •
Missing some Tweet in this thread? You can try to
force a refresh