Osterholm: "There is this viral interference."
Viral interference is a well-known (but poorly understood) phenomenon. Interference from rhinovirus is generally thought to have ended the swine flu epidemic in 2009.
thelancet.com/journals/lanmi…
thelancet.com/journals/lanmi…
This great short article from @m_soond explains the viral interference theory of flu vanishing when COV2 became epidemic.
medium.com/illumination-c…
medium.com/illumination-c…
If true, we would expect flu to return when COV2 has infected a large share of the population and recedes to endemicity.
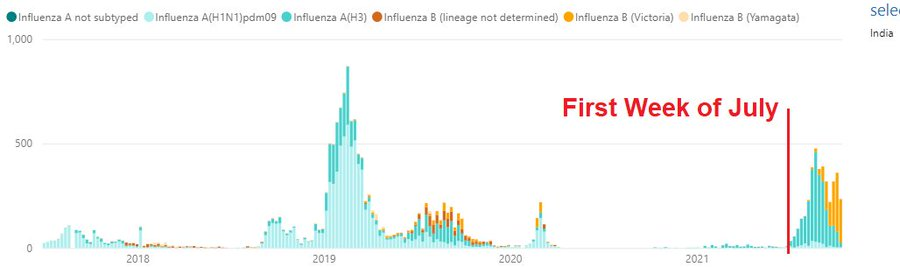
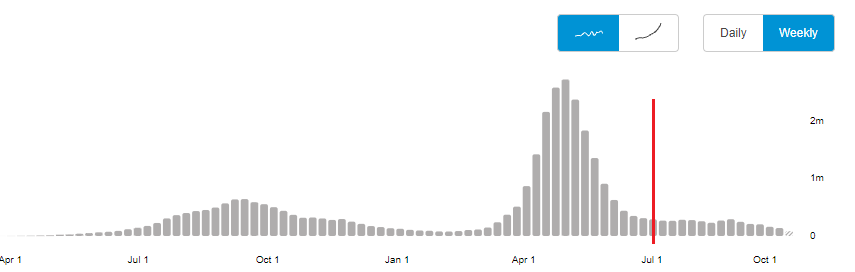
That may be happening in the Indian subcontinent.
Here are WHO charts for India for Flu and COV2 with the first week of July, 2021 marked.
That may be happening in the Indian subcontinent.
Here are WHO charts for India for Flu and COV2 with the first week of July, 2021 marked.
PLC has more on India and the rest of the subcontinent.
https://twitter.com/Humble_Analysis/status/1448307138955124742
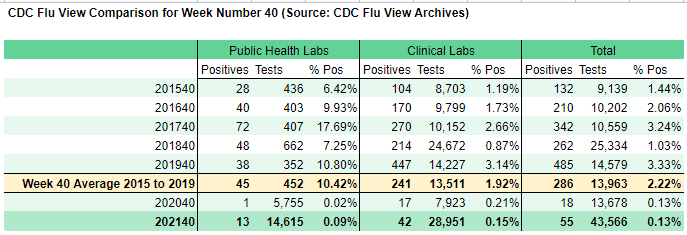
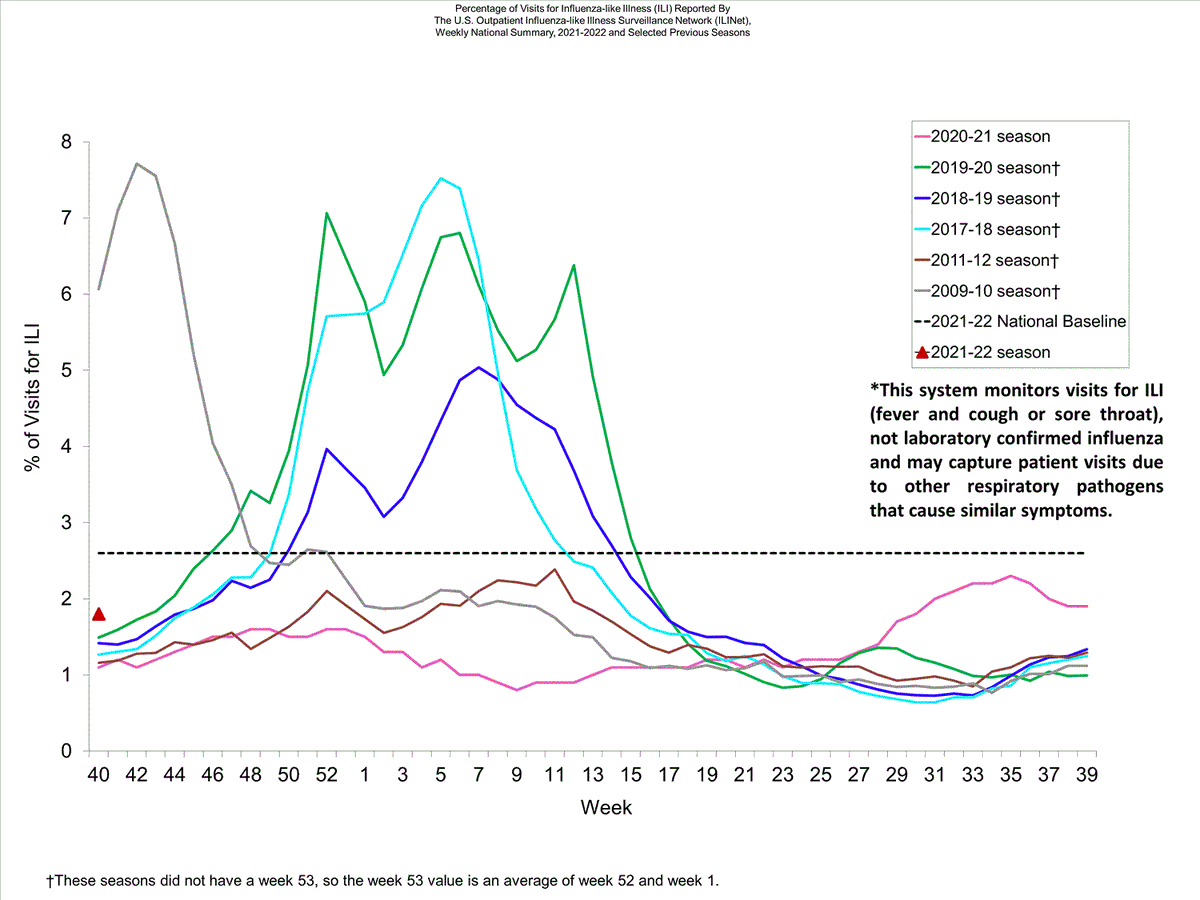
US outlook: Flu is still missing in all regions and it is possible the whole country will skip another flu year, as the southern hemisphere did; if flu does return to normal levels somewhere, it will likely be a signal that COV2 yielded and receded to endemic levels there.
Correction: New Zealand RSV wave peaked in July, their winter, so not out-of-season but larger than usual.
esr.cri.nz/our-services/c…
esr.cri.nz/our-services/c…

• • •
Missing some Tweet in this thread? You can try to
force a refresh