
Don’t miss a new accredited #tweetorial launching Monday here on @cardiomet_CE. Our newest core faculty member, #interventionalist & #SoMe education enthusiast @aayshacader will be discussing #antiplatelet tx in an oh-so-tough scenario--#cardiogenicshock complicating #STEMI.
FOLLOW US now and be there! @DLBHATTMD @DrMauricioCohen @SVRaoMD @HeartBobH @HeartOTXHeartMD @Heart_SCCT @TCTMD @GreggWStone @gabrielsteg @cpcannon @agtruesdell @evandrofilhobr @SCAI @SripalBangalore @mmamas1973 @SABOURETCardio @PCRonline @Pooh_Velagapudi #CardioTwitter
1) Welcome to a tweetorial on antiplatelet therapy for #STEMI in #cardiogenic shock #CS! Accredited for 0.50 credits by @academiccme! I am @aayshacader. Be sure to see prior tweetorials on this topic and still earn credit at cardiometabolic-ce.com/category/plate… 

2) This series is supported by educational grants from AstraZeneca, Bayer, and Chiesi. Faculty disclosures are listed at cardiometabolic-ce.com/disclosures/.
Let's start with a case!
Let's start with a case!
3) 56M w/DM, HTN presents w/anterior STEMI in cardiogenic shock; BP ~70/30 mmHg, HR ~ 120 bpm. Inotropes are started: he is in @SCAI Shock stage C. Cath lab activated for primary PCI. Meanwhile, he is extremely restless with ongoing chest pain. He’s given IV morphine.


4) With what would you preload this patient with prior to primary PCI?
A. Aspirin 300mg, clopidogrel 600mg both PO
B. Aspirin, 300mg,ticagrelor 180mg both PO
C. Aspirin 300mg, prasugrel 60mg both PO
D. Aspirin 300mg PO, IV Cangrelor
A. Aspirin 300mg, clopidogrel 600mg both PO
B. Aspirin, 300mg,ticagrelor 180mg both PO
C. Aspirin 300mg, prasugrel 60mg both PO
D. Aspirin 300mg PO, IV Cangrelor
5) The guidelines are clear on #DAPT in STEMI.
Oral non-enteric coated aspirin (150-300mg)
If unable to swallow, 75-150 mg IV aspirin
More potent P2Y12 blockers w/rapid onset of action (ticagrelor/prasugrel) preferred over clopidogrel
Eur Heart J. 2018;39(2):119-177
Oral non-enteric coated aspirin (150-300mg)
If unable to swallow, 75-150 mg IV aspirin
More potent P2Y12 blockers w/rapid onset of action (ticagrelor/prasugrel) preferred over clopidogrel
Eur Heart J. 2018;39(2):119-177

6) Antiplatelet agents are a therapeutic cornerstone in STEMI, during & after PCI. But, DAPT in #CS is largely understudied in RCTs. Effective & safe antithrombotic Rx in CS is challenging due to both patient & Rx-related factors. Eur Heart J Cardiovasc Pharmacother. 2021;7:125

7) Physical & pharmacokinetic impacts of CS ⬇️ effectiveness of oral antithrombotic Rx--impaired absorption, altered distribution, metabolism & excretion, co-administered Rx, targeted temperature mx(TTM) & use of MCS.
Oral P2Y12 inhibitors may also have CYP450 interactions
Oral P2Y12 inhibitors may also have CYP450 interactions
8) Here’s a detailed look at these pharmacokinetic mechanisms affecting antiplatelet drugs in cardiogenic shock & the critically ill.
Eur Heart J Cardiovasc Pharmacother. 2021;7(2):125-140.
Eur Heart J Cardiovasc Pharmacother. 2021;7(2):125-140.

9) Importantly, morphine & fentanyl, often given in STEMI, inhibit gastric emptying & delay absorption of oral P2Y12i's, increasing risk of ischemic events.
N Engl J Med. 2014 Sep 11;371(11):1016-27
Eur Heart J. 2016 Jan 14;37(3):245-52.
Thromb Haemost. 2018 Mar;118(3):601-612.
N Engl J Med. 2014 Sep 11;371(11):1016-27
Eur Heart J. 2016 Jan 14;37(3):245-52.
Thromb Haemost. 2018 Mar;118(3):601-612.
10) There are no RCTs of aspirin in CS.
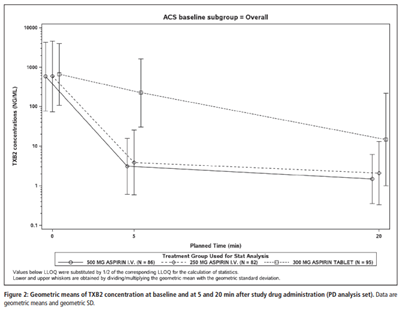
But in the ACUTE RCT, in ACS (5.5% STEMI), single dose 250 or 500mg IV ASA achieved faster & more complete inhibition of TXA2 generation & platelet aggregation, compared to oral 300mg, w/comparable bleeding.
Thromb Haemost 2017;117:625–635
But in the ACUTE RCT, in ACS (5.5% STEMI), single dose 250 or 500mg IV ASA achieved faster & more complete inhibition of TXA2 generation & platelet aggregation, compared to oral 300mg, w/comparable bleeding.
Thromb Haemost 2017;117:625–635
11) What about P2Y12 blockers? Again, no RCTs comparing them in #CS. Despite their greater potency, pharmacodynamic studies have shown a gap in their onset of action, especially in patients w/ STEMI or hemodynamic impairment.
12) Crushed ticagrelor (MOJITO study) & prasugrel (CRUSH study) may be better delivery routes.
J Am Coll Cardiol 2015;65: 511–512
J Am Coll Cardiol 2016;67:1994–2004
But, to really cover the lag time before onset of action of oral P2Y12i’s in #CS you likely need something IV.
J Am Coll Cardiol 2015;65: 511–512
J Am Coll Cardiol 2016;67:1994–2004
But, to really cover the lag time before onset of action of oral P2Y12i’s in #CS you likely need something IV.
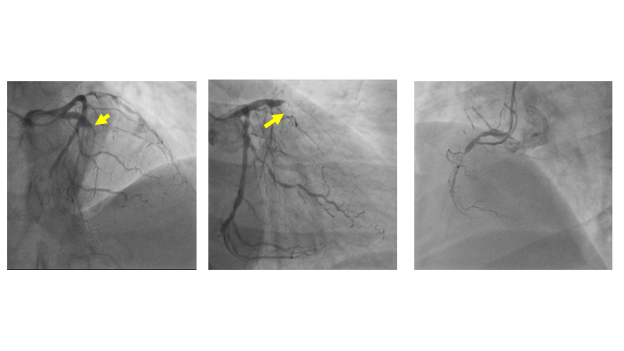
13) Anyway, back to our patient. This is his coronary angiogram. His BP is maintained with inotropes. There’s huge thrombus burden at an occluded ostioproximal LAD, a significantly diseased principal OM & diffusely diseased mid RCA with distal occlusion.
What would you do?
What would you do?
14) Poll:
1) Wire, direct stent only LAD
2) Aspirate thrombus, then stent LAD
3) Aspirate, IC Eptifibatide & stent LAD
4) Aspirate, IV Cangrelor & stent LAD
Pls mark your answer & come back tomorrow for the answer and more education! @manesh_patelMD @ziadalinyc @ToddVillinesMD
1) Wire, direct stent only LAD
2) Aspirate thrombus, then stent LAD
3) Aspirate, IC Eptifibatide & stent LAD
4) Aspirate, IV Cangrelor & stent LAD
Pls mark your answer & come back tomorrow for the answer and more education! @manesh_patelMD @ziadalinyc @ToddVillinesMD
15) Welcome back to this #tweetorial on antiplatelet tx in STEMI+CS. I am @aayshacader
We got very limited flow after wiring w/huge thrombus burden. So we performed thrombus aspiration for this pt, then DES stenting. But remember, this is reserved for exceptional circumstances
We got very limited flow after wiring w/huge thrombus burden. So we performed thrombus aspiration for this pt, then DES stenting. But remember, this is reserved for exceptional circumstances

16) Routine use of thrombectomy is not recommended (Class III) in STEMI (Eur Heart J. 2018;39(2):119-177).
(This is based on TOTAL: J Am Coll Cardiol. 2018;72(14):1589-1596 & TASTE trials: Engl J Med. 2013 Oct 24;369(17):1587-97)
(This is based on TOTAL: J Am Coll Cardiol. 2018;72(14):1589-1596 & TASTE trials: Engl J Med. 2013 Oct 24;369(17):1587-97)

17) We went ahead and stented his LAD after some predilatation. This is what it looked like soon after stenting. He was doing well with inotropic support. No chest pain.

18) But STEMIs are always full of surprises. The next shot revealed this⤵️: every IC’s nightmare

19) What would you do now?
a) IV Cangrelor
b) IC GPIIb/IIIa inhibitors
c) More IC heparin
d) Increase inotropes and see
Please vote!
a) IV Cangrelor
b) IC GPIIb/IIIa inhibitors
c) More IC heparin
d) Increase inotropes and see
Please vote!
20) Our patient developed no reflow. A lot of things might’ve caused it, but damage control first, with what we’ve got. In addition to IC nicardipine & nitroglycerin, we gave him IC eptifibatide bolus (a GPIIb/IIIa inhibitor) & continued infusion, which rectified the situation.
21) Let’s look at the role of IV GPIIb/IIIa inhibitors. There are 3GPI’s: abciximab, eptifibatide and tirofiban.
GPI’s bind to GP IIb/IIIa platelet receptor, blocking the final common pathway of platelet aggregation. Here too, there isn’t much RCT evidence in the setting of CS
GPI’s bind to GP IIb/IIIa platelet receptor, blocking the final common pathway of platelet aggregation. Here too, there isn’t much RCT evidence in the setting of CS

22) Existing STEMI guidelines state that GPIs may only be considered (Class IIa) for bailout in case of thrombotic complications or no reflow. They have increased bleeding risk & are not for routine upstream use in STEMI. Eur Heart J. 2018;39(2):119-177

23) In the PRAGUE-7 RCT no benefit of routine pre-procedural abciximab was seen compared to its selective use in STEMI patients with cardiogenic shock undergoing primary PCI. (Acute Card Care. 2011 ;13(3):116-22)

24) However, a recently published ESC Thrombosis WG/ACCA/EAPCI consensus document for ACS in CS & #OHCA suggests considering GPI as a bridge to achieve sufficient platelet inhibition while awaiting onset of oral Rx in CS & OHCA.
Eur Heart J Cardiovasc Pharmacother 2021;7:125
Eur Heart J Cardiovasc Pharmacother 2021;7:125

25) They also refer to concerns of oral P2Y12i interactions w/ #fentanyl infusions, given to unstable #CS patients who might be ventilated. Theoretically, fentanyl may delay oral P2Y12i absorption much more than peri-PCI morphine. Eur Heart J Cardiovasc Pharmacother 2021;7:125
26) Looking back at what happened: our pt got ticagrelor loading & also received morphine for ongoing chest pain. Recall the interactions of morphine with oral P2Y12i’s. This may have contributed to the no reflow we saw in this pt, in addition to huge de novo thrombus burden.
27) Interestingly, a recent observational study of short-duration tirofiban in morphine-treated STEMI pts showed significant ⬇️ acute stent thrombosis, w/acceptable bleeding penalty... but larger & prospective studies are warranted.
(Platelets 2020;31: 174–178)
(Platelets 2020;31: 174–178)

28) Knowing what we know now, in an ideal world, what might have been the best antiplatelet loading protocol (+ASA) for this shock pt?
Mark your answer & return for the last take tomorrow!
Mark your answer & return for the last take tomorrow!
29) Welcome back! You are just a few clicks away from 0.5h CE/#CME credit--#physicians #nurses #pharmacists! I am @aayshacader and we are learning about optimal #antiplatelet tx in a case of #STEMI complicated by #cardiogenicshock. Thanks for joining us!
30) We’ve learnt about oral P2Y12 inhibitors and IV GPIs; all have been around for a while. The new(er) kid on the block is IV Cangrelor. And that’s your answer.
Ther Adv Cardiovasc Dis. 2019;13:1753944719893274.
Ther Adv Cardiovasc Dis. 2019;13:1753944719893274.

31) Cangrelor is the only IV P2Y12 inhibitor. it has been extensively studied in the CHAMPION trials for pre, peri & post-PCI. We could have given him Cangrelor upfront at the start of PCI, or when we noted peri-procedural complication of no reflow.

32) Now, which of the following re: Cangrelor is false?
A. Rapid onset & offset of action
B. Can be used as a “bridge”
C. Interacts with opiates
D. No interaction with CYP-450
Please vote!
A. Rapid onset & offset of action
B. Can be used as a “bridge”
C. Interacts with opiates
D. No interaction with CYP-450
Please vote!
33) Cangrelor is a nonthienopyridine ATP analog. It reversibly binds the P2Y12 receptor, has a short half-life, a rapid onset & offset of action. It has no CYP interactions. As it’s given IV, there are no interactions with opiates either.


34) Some more insight into its pharmacokinetics: The CANTIC trial showed that the addition of #cangrelor leads to prompter & more potent platelet inhibition compared with crushed #ticagrelor alone, in STEMI patients undergoing primary PCI.

35) 2 reasons why CANTIC trial is pivotal:
- It showed that #cangrelor can bridge the gap in platelet inhibition compared with crushed oral P2Y12 inhibitors
- No drug–drug interaction w/ #ticagrelor allows a more versatile use with respect to timing of its administration
- It showed that #cangrelor can bridge the gap in platelet inhibition compared with crushed oral P2Y12 inhibitors
- No drug–drug interaction w/ #ticagrelor allows a more versatile use with respect to timing of its administration
36) The use of Cangrelor as a bridge to avoid surgical delays is especially important in STEMI shock cases. Some of them might be in shock due to mechanical complications of STEMI such as free ventricular wall rupture/ ventricular septal defects & need emergent surgery.
37) So, had we used Cangrelor, a switch to oral P2Y12 blockers would’ve been necessary as maintenance #DAPT, in addition to ASA. This would require a loading dose of oral P2Y12 inhibitors. Ticagrelor is the P2Y12 agent of choice here, because there are no DDIs between the two.
38) So, when and how do we load?
Here's a neat guide:
Here's a neat guide:

39) Our patient recovered well w/periprocedural IC GPI bolus & IV infusion, w/no bleeding episodes. He was maintained on ticagrelor 90mg BD with aspirin 75 mg OD. Inotropes were tapered.
But, in cases of more severe shock, there may be need for circulatory/ LV assist devices.
But, in cases of more severe shock, there may be need for circulatory/ LV assist devices.
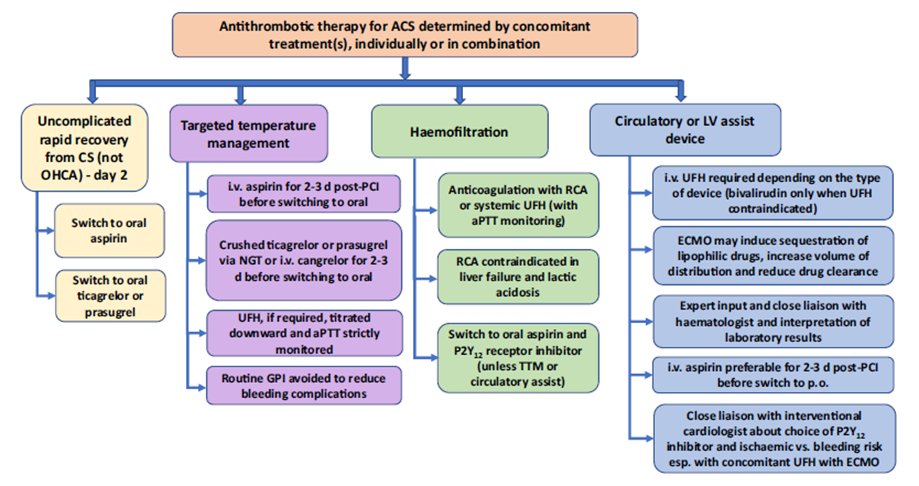
40) These are notorious for both bleeding & ischaemic complications- often occurring simultaneously. Here, greater attention to detail, to maintain a fine balance between the many antithrombotic therapies, is needed. Here’s a neat summary of action points in more complicated CS.
41) As we said earlier, DAPT in STEMI with CS is under-studied by RCTs. Most recommendations for this subset are derived from the more general STEMI trials. The DAPT-SHOCK-STEMI multicentre RCT, currently recruiting, may have some answers. clinicaltrials.gov/ct2/show/NCT03…
42) Here, 304 AMI pts w/CS & treated w/primary PCI are randomised 1:1 to:
-IV cangrelor (bolus 30 μg/kg ->infusion 4 μg/kg/min) vs
-oral ticagrelor
Primary clinical endpoint: 30-day MACE (Death/MI/Stroke)
Laboratory endpoint: peri-procedural platelet inhibition (PRU< 50%)
So:
-IV cangrelor (bolus 30 μg/kg ->infusion 4 μg/kg/min) vs
-oral ticagrelor
Primary clinical endpoint: 30-day MACE (Death/MI/Stroke)
Laboratory endpoint: peri-procedural platelet inhibition (PRU< 50%)
So:
43) That’s it from us. This case of STEMI in shock has taken us on a long ride and there are more data from focused trials to come! For now, I am @aayshacader, I THANK YOU for joining us, & I invite u to go to cardiometabolic-ce.com/plts9 and claim your credit!

• • •
Missing some Tweet in this thread? You can try to
force a refresh












