We can compare the UK experience to other similar countries to understand the role of public health rules in limiting disease.
Here I choose the Netherlands for comparison since it is close geographically, has similar vaccine rates, and had an initial Delta surge of similar size
Here I choose the Netherlands for comparison since it is close geographically, has similar vaccine rates, and had an initial Delta surge of similar size

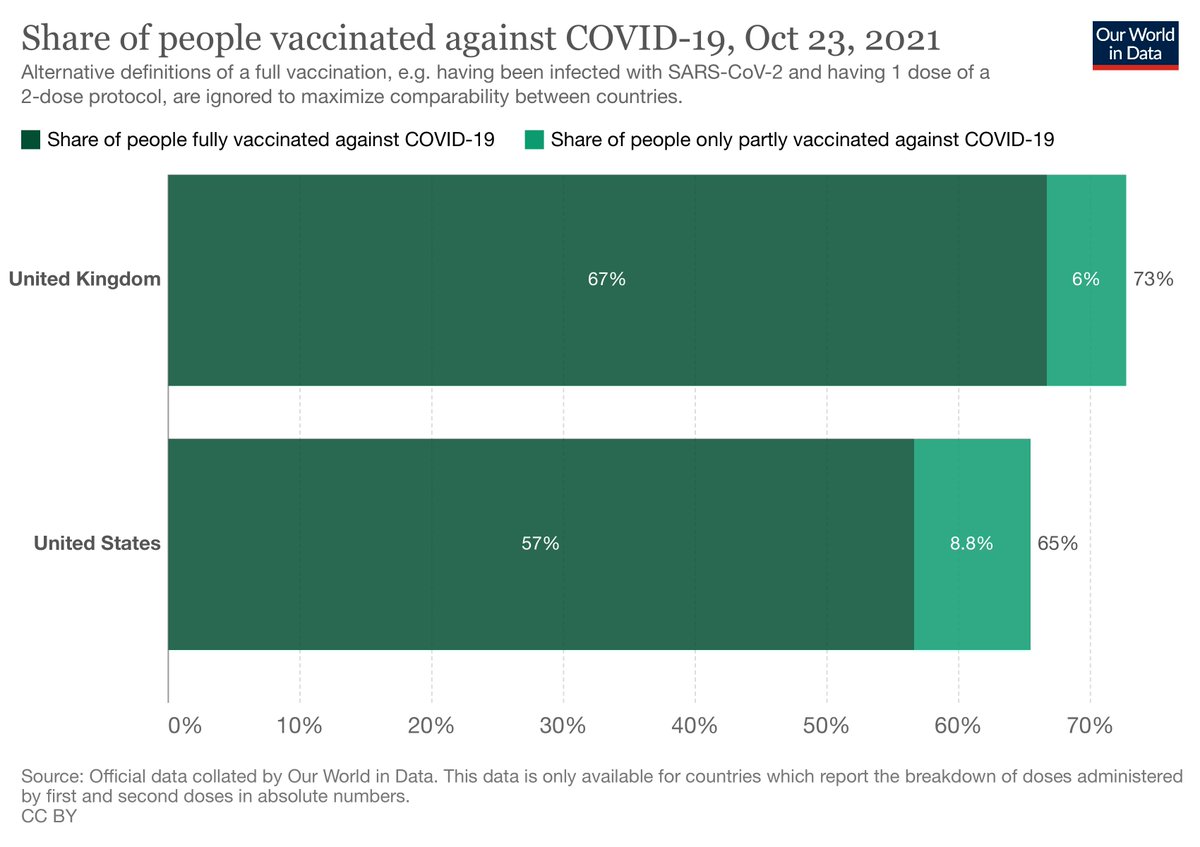
As apparent from the graph above, UK doesn't come out too well. But first let's establish the conditions. Vaccination rates are similar between UK and Netherlands

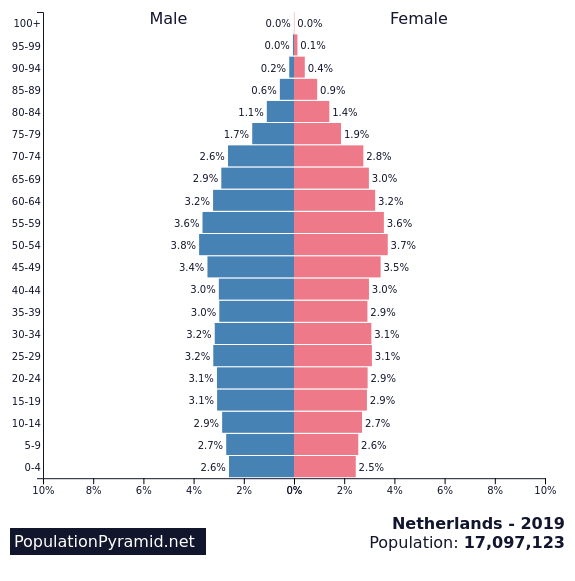
Age structure is similar with the Netherlands having slightly more people in age segments >50yo

Urbanization is similar


So UK and Netherlands are pretty good pair of countries to compare. There may even be some cultural similarities around enthusiasm for football, bars, and nightclubs, but I'm not an expert there and will let others comment.
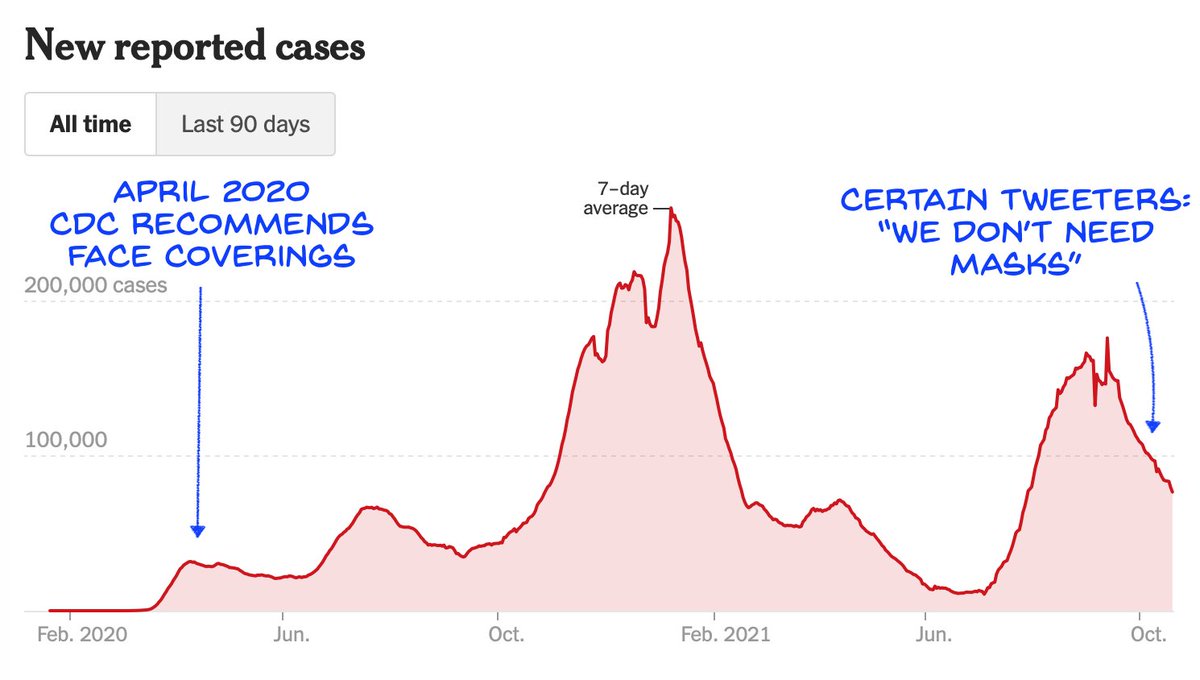
UK famously dropped all legal requirements for indoor masks and business density on July 19. Masks were still encouraged on public transport, but actual mask usage was less than 50%
theguardian.com/world/2021/sep…
theguardian.com/world/2021/sep…
Netherlands had dropped indoor mask requirements in June but kept public transport mask requirements, and in Amsterdam masking remained common (it was still required in city buildings for example)
webcache.googleusercontent.com/search?q=cache…
webcache.googleusercontent.com/search?q=cache…
On July 9, the Netherlands reintroduced density restrictions and a curfew, in response to data that most infections were in nightlife settings, so that's essentially the opposite of UK moving from restrictions to none on July 19
axios.com/netherlands-re…
axios.com/netherlands-re…
The Netherlands started requiring vaccine proof to enter restaurants, bars, concerts etc on September 25 in lieu of capacity restrictions, whereas UK still has neither
reuters.com/business/healt…
reuters.com/business/healt…
So overall we can consider the Netherlands restrictions as quite liberal (it wasn't universal indoor masking or a ban on indoor dining) and expect them to allow a certain level of disease, but we'd expect the UK's complete lack of restrictions to allow even more disease.
And that's what we see. The difference between the UK and the Netherlands in August is quite noticeable. It's not black and white, but it's significant. We can look at other countries, and UK continues to be an outlier, although other countries have bigger societal differences.

On first glance, if one doesn't think about the time lag between an infection event and when it gets diagnosed, or the ramp-up time in behavioral changes, it would seem that the drop in UK cases after July 21 was due to *removing* restrictions, but logic says that's not likely
Likewise a naive person would say adding restrictions on July 7 caused a rise in infections over the next week, but again we'd expect those cases to have occurred prior to the restrictions being implemented.
In practice we tend to see a 2-week lag between a new policy and expected effects. Not sure why. Maybe policy implementation takes a week, or maybe testing behavior is "sticky": when cases are rising, people may be fast to test; when cases are dropping they may be slow to test.
This seems to have tripped up the Economist, who declared victory in UK at exactly the wrong time: just 3 days before cases began rising again.
economist.com/britain/2021/0…
economist.com/britain/2021/0…
However the laws of biology do not dissipate just because people want them too. There are some mysteries to the virus, but its ability to infect unvaccinated people with high efficiency and also some vaccinated people at lower efficiency are not among them.
Neither do the laws of math and physics bend to the will of politicians. Fewer people breathing the same air means slower spread of disease. Absorption of viral particles on masks means fewer particles to seed infections.
Why bring this up now? Because it matters to how we approach the winter. We have a higher level of people unvaccinated than UK, while age structure is similar:

The 35% who are not vaccinated are mostly of younger ages. However that's only somewhat comforting to those older than 65. This group is highly vaccinated, but efficacy of the vaccine against hospitalization and death drops with age.
axios.com/age-coronaviru…
axios.com/age-coronaviru…
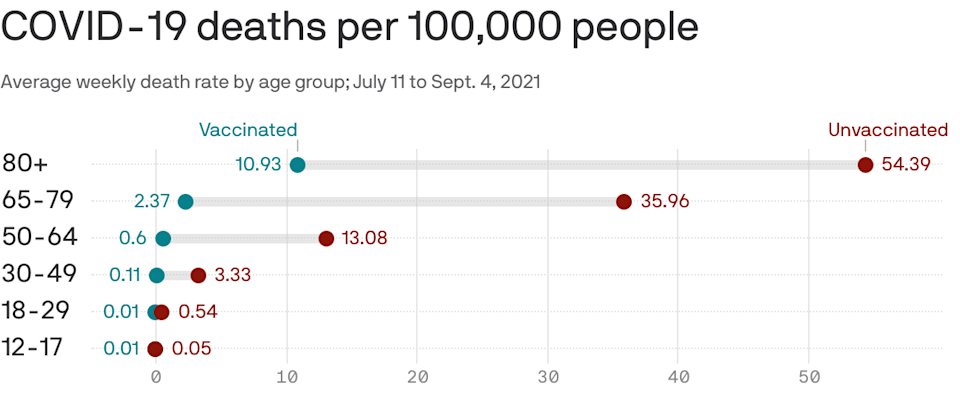
Thus reducing disease rates overall is still useful to protecting the most vulnerable.
It is also useful for preventing cases at schools until young kids can be vaccinated.
It is also useful for preventing cases at schools until young kids can be vaccinated.
Now what is the reason for the increase in cases in both UK and Netherlands in the last 2 weeks? I'm not sure but I couldn't identify any policy changes that would explain it (those who know can correct me), so I wonder if it's more people indoors with colder weather.
The implication for the US is that, if cases start rising again due to cold weather, then we would want to maintain or reintroduce measures such as masks in indoor spaces and vaccines for dining, to get cases flattened or trending downward again.
• • •
Missing some Tweet in this thread? You can try to
force a refresh