
1/ cdc.gov/coronavirus/20… After release of their MMWR study, CDC releases this BRIEF on Infection-induced vs. Vax-induced Immunity. It is a CONFUSED document – both accepting NI, but illogically recommending VAX anyway. This 🧵🧵 appraises the BRIEF –
2a/ It is important that the CDC get this STRAIGHT. For children 5-11 particularly, NI reduces C19 risk significantly, to the point that the vaccine offers virtually no benefit to COVID-recovered children. The ACIP meets tomorrow on this question. They NEED to address NI (PI)!
2b/ We will go through the document section by section, highlighting key takeaways and provide refutations/commentary if necessary.
3a/ Executive Summary: They essentially state both PI and and fully vaccinated (FV) have a “low risk” of subsequent infection. I am glad they finally acknowledge this. This is a big “baby step” for them. 

3b/ They then state that Ab' not informative enough on the state of an indiv.’s protection. OK then – but why does @FDA @CDCgov accept Ab levels for “immunobridging” approval in the 5-11 yo ?? CANNOT have BOTH WAYS! Use for EUA application, but then dismiss use individually!
@FDA @CDCgov 3c/ They state vaccination leads to a more “consistent” antibody response – BUT WAIT, DIDN’T YOU JUST SAY antibody metrics are unreliable/untested ?? Literally contradict themselves within sentences of each other.
@FDA @CDCgov 3d/ They state certain elderly and immunocompromised persons may have decreased immunity following both infection and vaccination. Agreed completely. This argues AGAINST a mandate however, and FOR recommendations based on individual circumstance.
@FDA @CDCgov 3e/ They then state a “growing body of [evidence]” supports vaccination after infection. We will get to this, but essentially, they use their “KY” and recent MMWR study as the only CLINICAL studies supporting their position. What a coincidence!!!
@FDA @CDCgov 4/ BACKGROUND: “… approximately 1/2 of PI adults in the US have NOT BEEN VACCINATED.” It is clear they view the PI & children 5-11 as last refuge of the Unvax. They R honed in on achieving a political goal of universal VAX, NOT a public health goal of universal PROTECTION.
@FDA @CDCgov 5a/ Immune Response to Vaccination: A lot of basic science here regarding antibodies, with nothing particularly revealing. Basically their point is there is no standardization of Ab testing that is clinically useful.

@FDA @CDCgov 5b/They do acknowledge a “high-degree” of correlation between neutralizing [Ab] and overall decrease risk in infection, with 20% and 3% of MEAN CONVALESCENT (e.g. previously infected) levels correlating with 50% infection and hospitalization risk, respectively.
@FDA @CDCgov 5c/ Essentially because Ab levels or testing provide a “partial” pic of indiv., they state it c/n determine individual risk. As discussed earlier, this CIRCULAR LOGIC IS DIZZYING – relying on Ab's when CONVENIENT for approval on the MASSES , but dismissing it for INDVIDUALs use.
@FDA @CDCgov 5d/ BIG IDEA @CDC: Why not let a COVID-recovered person and their PHYSICIAN determine their individual levels of protection, and make the RIGHT decision for that person ? Nuance and EQUIPOISE is used for virtually every other disease --- why not COVID?
@FDA @CDCgov @cdc 6a/ Immune Response and Duration of Protection: Bottom line here, is the CDC FINALLY ACKNOWLEDGES SEVEN studies showing 80-93% protection for up to 12 months, without any decline!!

@FDA @CDCgov @cdc 6b/ They then note that most (5/7) of these studies were retrospective, and outline BIASES of the study design. Interesting, considering their own MMWR studies are highly BIASED!
@FDA @CDCgov @cdc 6c/ But then they go on to highlight one PROSPECTIVE cohort study of 25,000 HCWs, which found 84% protection against overall infection. SOUNDS LIKE THEY UNDERSTAND THE EFFECTIVENESS OF NATURAL IMMUNITY, then!
@FDA @CDCgov @cdc 6d/ They then note that these studies may not have addressed variants of concern (VOCs). So maybe PI is suboptimal for VOCs, right? Onward . . .
@FDA @CDCgov @cdc 6e/ Later, the document states “Multiple studies have found that [vax effectiveness] against hospitalization and/or severe disease continues to be high…84-96% up to 6 months following vaccination” So @CDC @CDCDirector WHAT’s the DIFFERENCE BETWEEN PI and VAX?
@FDA @CDCgov @cdc @CDCDirector 7/Variants of Concern- Nothing here really. A lot of discussion on laboratory evidence, which might be insightful, but not actionable. They concede reduced VE against DELTA, but hang onto its high effect on hospitalization and severe disease.
@FDA @CDCgov @cdc @CDCDirector 8a/ COMPARISON OF INFXN- and VAX-INDUCED IMMUNE RESPONSES:
They cite MY review/metanalysis paper (& @noorchashm ) that FOUND NO SIGNIFICANT DIFFERENCE between PI and Vax! I am glad they read it.
It is here: cureus.com/articles/72074….
They cite MY review/metanalysis paper (& @noorchashm ) that FOUND NO SIGNIFICANT DIFFERENCE between PI and Vax! I am glad they read it.
It is here: cureus.com/articles/72074….
@FDA @CDCgov @cdc @CDCDirector @noorchashm
https://twitter.com/mahesh_shenai/status/1454754411973124097?s=208b/Then counter this w/ recent MMWR Bozio study. They state study is from a network of 187 hospitals. This is an untrue embellishment. The study itself is only from 7 hosp, & 53% of the Vax group comes from 1 hosp. My critique of this FLAWED paper is here.
@FDA @CDCgov @cdc @CDCDirector @noorchashm 8c/ They then state that the MMWR study included more recent data then my systematic review. This too, is IINCORRECT. The MMWR study included PI from Oct 2020-Aug 2021. My study included 7 studies within this period, with 2 studies in April-August 2021.
8a-2/ Here is a screen shot of this most important section.
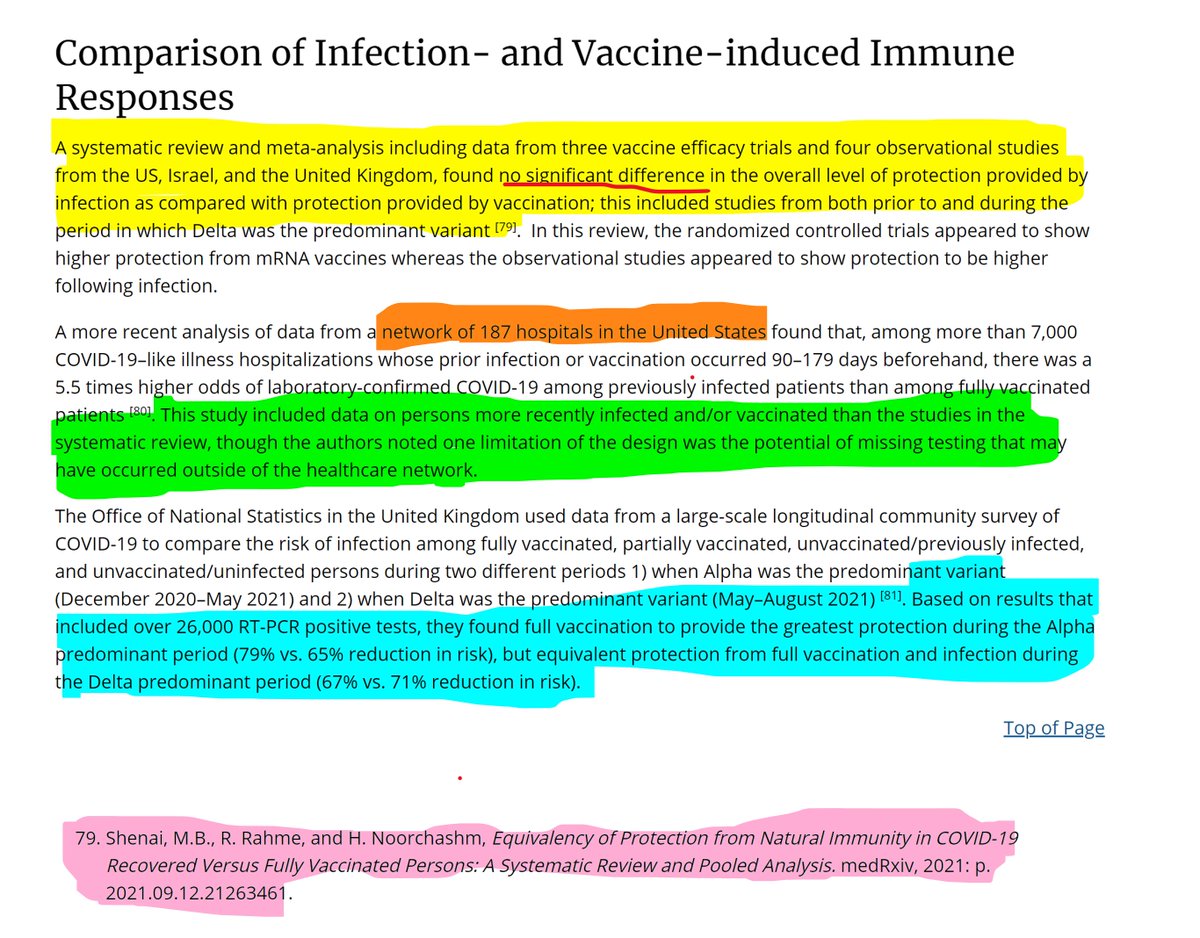
@FDA @CDCgov @cdc @CDCDirector @noorchashm 8d/ They then quote data from the UK, indicating that VAX provided better benefit (79% vs. 65%) during Alpha phase, but PI provided slightly better BENEFIT than VAX during DELTA (67%-71%)!! But in essence, they are both comparable.
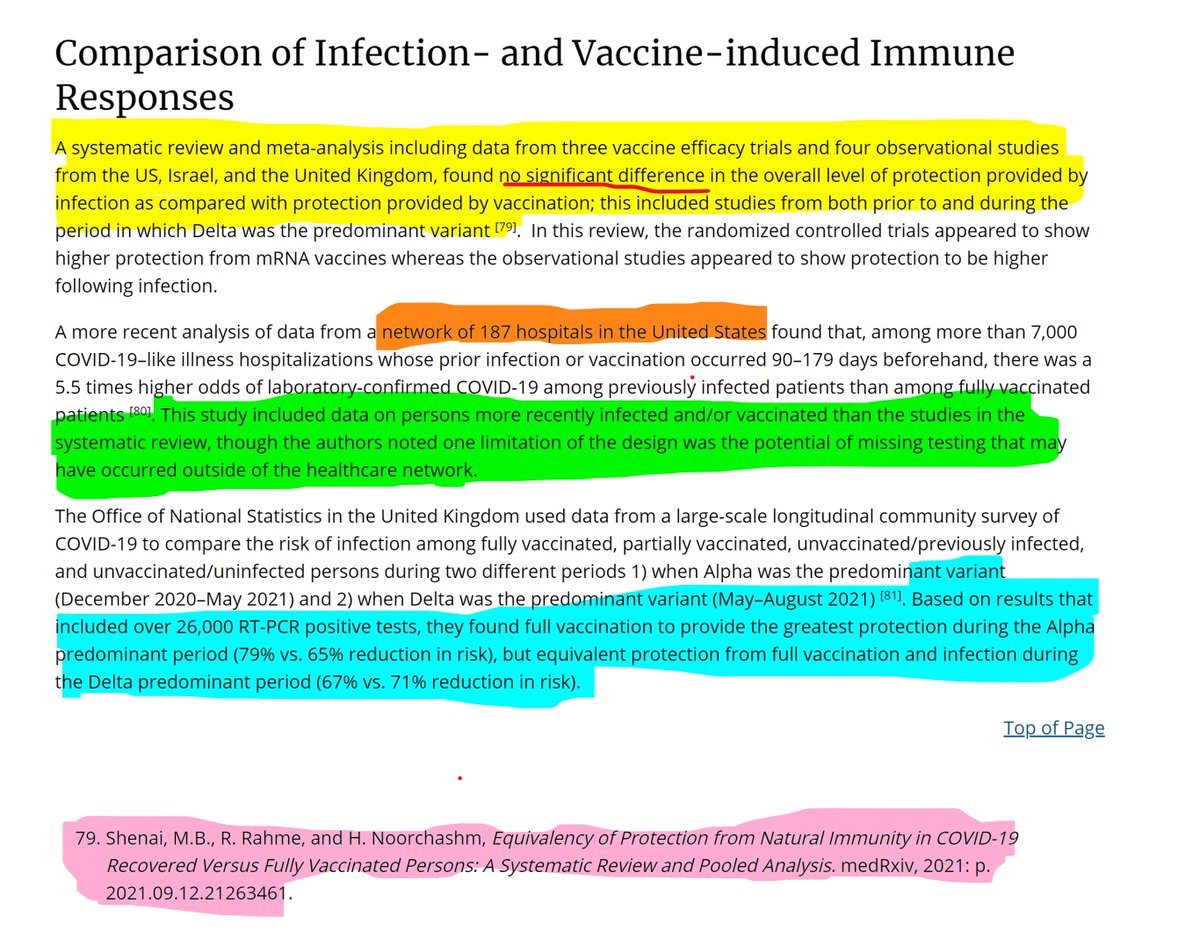
@FDA @CDCgov @cdc @CDCDirector @noorchashm 8e/ 🚩🚩🚩🚩 SO, bottom line: Outside of their own MMWR study, the PREPONDERANCE OF THE EVIDENCE STATES PI and VAX ARE AT SUBSTANTIVELY SIMILAR IN LEVELS OF PROTECTION !!!
@FDA @CDCgov @cdc @CDCDirector @noorchashm 9a/ VAX-INDUCED IMMUNE RESPONSES AFTER PREVIOUS INFECTION: So, here they try to state that “substantial immunologic and increasing epidemiologic evidence” increases protection against subsequent illness in PI. EVIDENCE PLEASE?

@FDA @CDCgov @cdc @CDCDirector @noorchashm 9b/ In fact, the evidence from Pfizer and Moderna’s OWN trials show significant DECREASE IN VE, with subsequent papers AVOIDING publishing PI’s VE entirely.

@FDA @CDCgov @cdc @CDCDirector @noorchashm 10a/ RISK OF REINFECTION in UNVAX vs. VAX IN PI: This is a disastrous section for this BRIEF. They state that “most but not all” studies show a benefit of vaccination. But in their citations, only their own “FLAWED” KY study clearly supports vax in PI

@FDA @CDCgov @cdc @CDCDirector @noorchashm 10b/ They take note of a Cleveland Clinic Study (Shrestha et al.) which demonstrated in a series of 2600 HCWs, NOT A SINGLE PERSON w/ PRIOR INFXN WAS REINFECTED, VAXXED OR NOT.
@FDA @CDCgov @cdc @CDCDirector @noorchashm 10c/ Then they bring up their MMWR “KY” study w/ multiple flaws, focused only on 246 reinfected persons, out of nearly 250,000 previously infected people. The study cites the RELATIVE ODDS ratio (2.3x) of reinfection, but gloss over the tremendously small absolute risk (0.09%).
@FDA @CDCgov @cdc @CDCDirector @noorchashm 10d/ The KY study has a number of other flaws, including it being a “case control” design, lack of a “test-negative” control, to mention a few.
@FDA @CDCgov @cdc @CDCDirector @noorchashm 10e/ Finally, they cite the Israeli Gazit study showing ~50% benefit of ONE dose vaccination in the PI. Interesting that they cite the vax benefit, BUT FAIL TO DISCUSS THE SAME STUDY FOUND A 6-27x benefit of PI vs. VAX !!! WHY CHERRY-PICK a RESULT from the SAME STUDY ???
@FDA @CDCgov @cdc @CDCDirector @noorchashm 10f/ Next is a study from India (Murugesan) et al. CDC concludes from this study that “overall risk of infxn was lowest among those that were vaxxed following infection.” What they FAIL to state is the improvement was small 86% vs. 91%, and statistically insignificant.

@FDA @CDCgov @cdc @CDCDirector @noorchashm 10g/ The same Indian study ALSO found that the VE for FV persons without history of PI was only 31.8%%. So in other words PI (86%) >> Vax (32%). Seriously . . .
@FDA @CDCgov @cdc @CDCDirector @noorchashm 10h/ Finally, this study STUDIED the wrong VACCINE! It looked at ChAdOx1 which was available in India (not in US), not the Pfizer or Moderna vax. So frankly, this study is not even GERMANE to the US conversation.
@FDA @CDCgov @cdc @CDCDirector @noorchashm 11a/ CONCLUSIONS. Reading through this brief carefully, shows the CDCs CONFUSION on the subject. They now SEEM to acknowledge the power of NI – yet still FAIL to grasp the essence of the evidence. And they still FAIL to CHANGE their policy stance on requiring vax in PI.
@FDA @CDCgov @cdc @CDCDirector @noorchashm 11b/ The only pieces of evidence they can cite in favor of their position, are their OWN studies in the MMWR, KY and the most recent study. Literally, these are the ONLY studies that are strongly in favor of vax in PI. Coincidence ?
@FDA @CDCgov @cdc @CDCDirector @noorchashm 11c/ The timing of this BRIEF, released the same day as the MMWR study is fascinating. It’s as if they commissioned that study to create the ONLY single study that unequivocally favors vax over PI. Creating evidence based on a conclusion, rather than vice versa.
@FDA @CDCgov @cdc @CDCDirector @noorchashm 11d/ But even in this BRIEF, the evidence they cite, taken and interpreted independently, clearly acknowledges the efficacy of prior infection. It is time that the @CDC @CDCDirector does as well.
@FDA @CDCgov @cdc @CDCDirector @noorchashm 11e/ Next up is our children at tommorow's ACIP. Please, for their sake, do the right thing and FINALLY acknowledge natural immunity. COVID-recovered children have a different benefit-risk calculus!
@FDA @CDCgov @cdc @CDCDirector @noorchashm 11e/ Thank you for reading. As always, open to any comments/corrections/concerns!
• • •
Missing some Tweet in this thread? You can try to
force a refresh





