
1/It is bad that clinician performance on matters related to the opioid crisis is *still* being measured in terms of # of opioid prescriptions.
These metrics, which ape prior metrics that drove the original⬆️ reject the approach we normally require for measuring quality of care
These metrics, which ape prior metrics that drove the original⬆️ reject the approach we normally require for measuring quality of care
https://twitter.com/DrZackaryBerger/status/1455556202583232523
2. To be clear. Optimal health care metrics require
a) clear denominator of eligible patients with the condition
b) clear evidence that the treatment's provision is wholly good or its nonprovision wholly bad
c)evidence that imposing the metric leads to improvements in health
a) clear denominator of eligible patients with the condition
b) clear evidence that the treatment's provision is wholly good or its nonprovision wholly bad
c)evidence that imposing the metric leads to improvements in health
3. For example, a metric such as "provision of cervical cancer screening" would be BAD if it includes persons with no cervix either because of hysterectomy, or because they are cis-male.
4/But not all acute or chronic pains are the same in every patient, leaving us without a homogeneous denominator. Even with chronic pain, the history, level of ability/disability, and access to alternatives should influence the what's right. From my talk: 

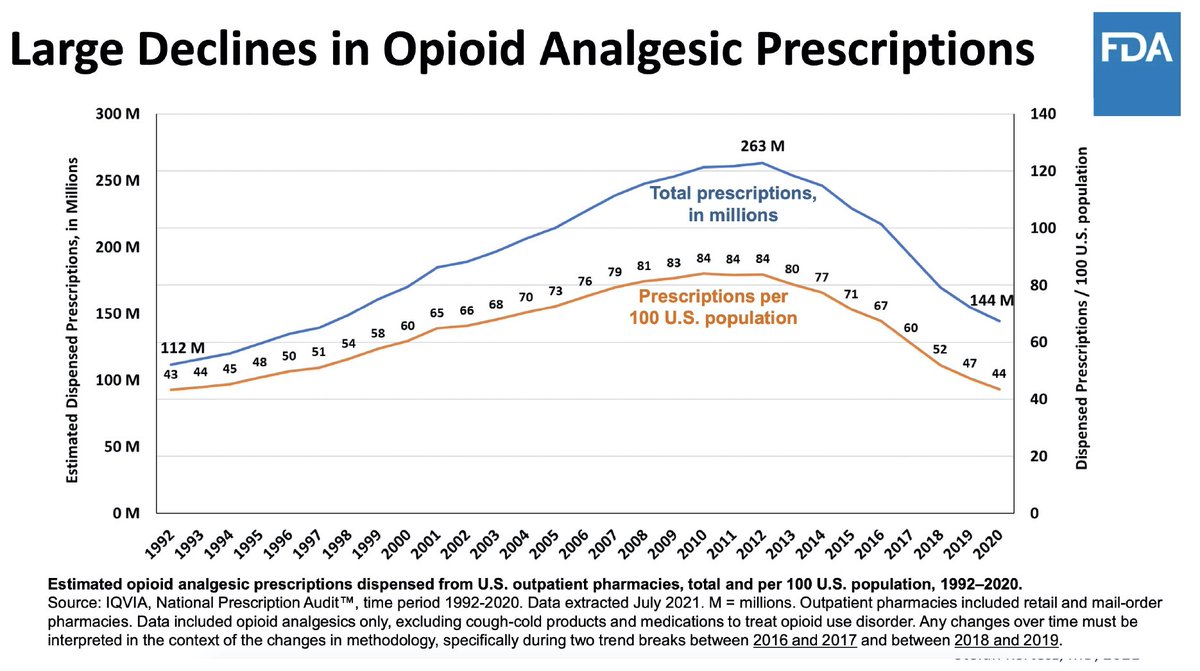
5/Of course, we know well that our opioid Rx run-up from mid 1990s to 2012 was driven by simplistic monotonic logic in which all pain was kind of "lumped together" commercially, all outcomes coned down simplistically. @DopesickOnHulu @papergirlmacy @AJ_Gordon
6/But the actual game of "make this opioid prescription number go down no matter what" is at odds with how we normally choose metrics.
No clarity on denominators.
No *evidence that making the # ⬇️protects the patient* (copious signals of harm)
But it's actually worse than that
No clarity on denominators.
No *evidence that making the # ⬇️protects the patient* (copious signals of harm)
But it's actually worse than that
7/What's "worse" is not that Rx opioid ⬇️is always harmful (not true!) Rather, it's a justice issue
Where there's harm, there's minimal effort to report or stop it.Why?Affected persons are disabled, lack political power & are stigmatized by powerful voices bendbulletin.com/lifestyle/heal…
Where there's harm, there's minimal effort to report or stop it.Why?Affected persons are disabled, lack political power & are stigmatized by powerful voices bendbulletin.com/lifestyle/heal…

8/A health system that has believes they might have excess prescription could:
/Assess the matter holistically, using internal data and speak to all stakeholders to understand it
/Consider promoting programs that tailor care with better service rather than blunt force metrics
/Assess the matter holistically, using internal data and speak to all stakeholders to understand it
/Consider promoting programs that tailor care with better service rather than blunt force metrics
9/We have suggested a set of "better (ie credible, patient-centered) metrics" for health systems seeking to assess the impact of their opioid deimplementation - published with @BethDarnall @AllysonVarley Megan McCullough in @JournalGIM link.springer.com/article/10.100…

10/At a time where today's opioid Rx/capita is at 1992 levels, and mg/capita at 2002, and overdoses worse, and patients abandoned, health leaders can reassess previously adopted metrics.
Protection of patients requires (a) respect for evidence; (b) listening (c) ethics /fin
Protection of patients requires (a) respect for evidence; (b) listening (c) ethics /fin
11/the above discussion may be of interest to many folks involved in the @DopesickOnHulu discussion from today or in opioid policy more generally @AJ_Gordon @DrSarahWakeman @gertner_alex @lipiroy @papergirlmacy @LeoBeletsky @ZachWritesStuff @ArtL7 @HillPharmD @national_pain
• • •
Missing some Tweet in this thread? You can try to
force a refresh











