So, the FORTE trial was recently published. This is a great trial, and there are many important lessons/concepts/questions that arise from this, which I wanted to highlight in this 🧵
sciencedirect.com/science/articl…
#mmsm
sciencedirect.com/science/articl…
#mmsm

So lets first understand the trial design.
There are two randomizations.
First randomization assesses different types of induction strategies, and lets first focus on that.
There are two randomizations.
First randomization assesses different types of induction strategies, and lets first focus on that.
Demographics- anything important to note?
See table-
High-risk are well represented, but important to note Gain 1q (which isnt a good player by any means, just not a part of R-ISS high-risk staging), does inflate overall number of HIGH-RISK to almost 60% of enrolled pts!
See table-
High-risk are well represented, but important to note Gain 1q (which isnt a good player by any means, just not a part of R-ISS high-risk staging), does inflate overall number of HIGH-RISK to almost 60% of enrolled pts!

As you can see in figure:
Three arms, one gets carf/cy/dex followed by auto, other carf/len/dex followed by auto, and third carf/len/dex with no auto.
Three arms, one gets carf/cy/dex followed by auto, other carf/len/dex followed by auto, and third carf/len/dex with no auto.

Alright- time for results!
But wait-
Before we dig into results, always best to stay grounded and think of what the trial was powered to ask/what primary endpoint is. Primary endpoint of first randomization is rates of very good partial remission. Need to keep it real here!
But wait-
Before we dig into results, always best to stay grounded and think of what the trial was powered to ask/what primary endpoint is. Primary endpoint of first randomization is rates of very good partial remission. Need to keep it real here!
Okay- finally results.
In KRd arm- 70% achieved at least VGPR after induction
In KCd arm- 54% achieved at least VGPR after induction.
This is line with previous data that imid based induction leads to higher response rates compared to cytoxan. No surprise.
In KRd arm- 70% achieved at least VGPR after induction
In KCd arm- 54% achieved at least VGPR after induction.
This is line with previous data that imid based induction leads to higher response rates compared to cytoxan. No surprise.
Okay, even though its not primary endpoint, what we all are really curious about is MRD rates after transplant/consolidation in the three arms. Lets be real.
Thats where the interesting stuff is!
Thats where the interesting stuff is!
So at first MRD 10-5 rates (prior to maintenance initiation) were actually comparable in KRD-cons arm compared to KRD-auto arm.
KCd= 43%
KRd-cons=56%
KRd-auto= 62%
Did additional KRd avert the need for auto? Had we finally laid rest to auto?!
Not so fast.
KCd= 43%
KRd-cons=56%
KRd-auto= 62%
Did additional KRd avert the need for auto? Had we finally laid rest to auto?!
Not so fast.
The KRd auto maintained MRD neg rates the best over time!!!
1 year sustained MRD rates:
KCd=25%
KRd=35%
KRd-Auto=47%
We have a winner!
Umm- it is not the primary endpoint, but still lots to process.
1 year sustained MRD rates:
KCd=25%
KRd=35%
KRd-Auto=47%
We have a winner!
Umm- it is not the primary endpoint, but still lots to process.
So what we learn:
-A single point of MRD negativity can be deceptive, and many patients lose it over time.
-With auto transplant, more patients kept their MRD negative status, something additional consolidation cycles with KRd couldnt do!
Auto still the KING for eligible pts!
-A single point of MRD negativity can be deceptive, and many patients lose it over time.
-With auto transplant, more patients kept their MRD negative status, something additional consolidation cycles with KRd couldnt do!
Auto still the KING for eligible pts!
I dont want to delve too much into this, this analysis wasnt powered for PFS and maintenance had a separate randomization but-
4 year PFS
69% with KRd/auto
56% with KRd12
51% with KCd.
4 year PFS
69% with KRd/auto
56% with KRd12
51% with KCd.
Please note-there is no VRD control, so we cannot say whether KRd is better than VRD based on this trial.
In two randomized trials in newly diagnosed (ENDURANCE and CLARION), K not better than V. Maybe, there is niche for high risk with K, biologically plausible? Not sure.
In two randomized trials in newly diagnosed (ENDURANCE and CLARION), K not better than V. Maybe, there is niche for high risk with K, biologically plausible? Not sure.
OKAY--
Now lets move on the next randomization!!
After completing consolidation, patients underwent a second randomization- either lenalidomide maintenance (which is standard of care) or carfilzomib+lenalidomide maintenance!
Now lets move on the next randomization!!
After completing consolidation, patients underwent a second randomization- either lenalidomide maintenance (which is standard of care) or carfilzomib+lenalidomide maintenance!

What was the endpoint of this randomization?
PFS.
Philosophically, I struggle with PFS as endpoint for maintenance, as it is logical additional therapy will delay progression. Does it change the overall course? We need OS for that.
The bar for maintenance tx should be OS.
PFS.
Philosophically, I struggle with PFS as endpoint for maintenance, as it is logical additional therapy will delay progression. Does it change the overall course? We need OS for that.
The bar for maintenance tx should be OS.
TIME FOR RESULTS!
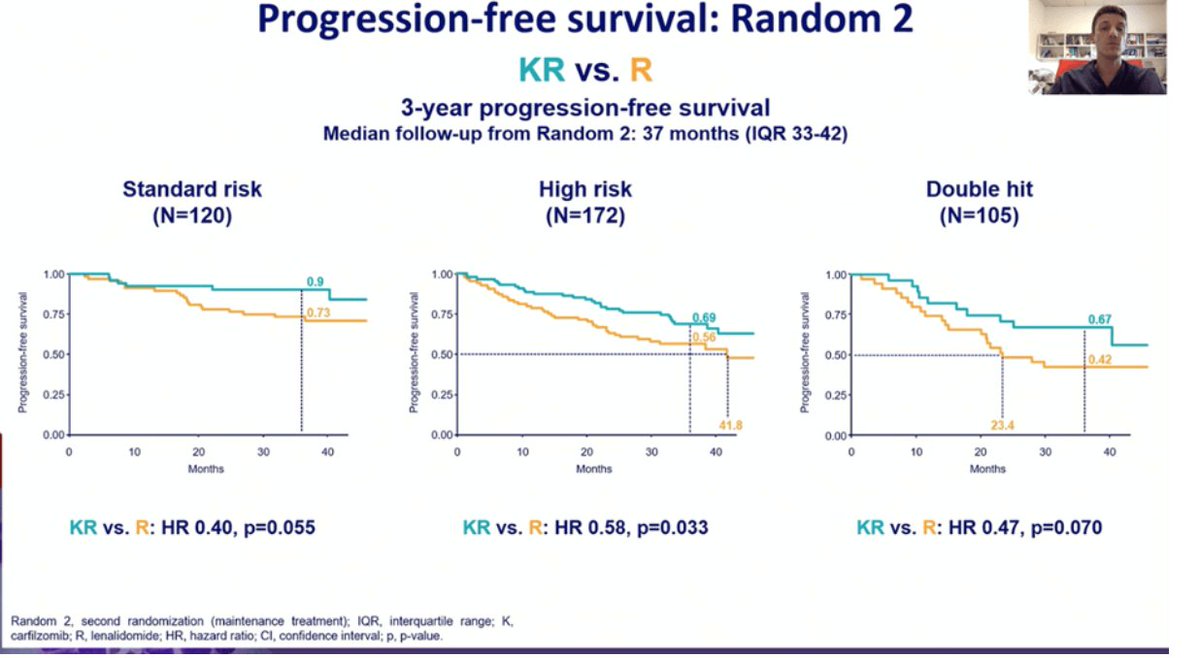
No surprise that additional therapy with an active drug led to improved PFS frankly, but 3 year PFS were 75% versus 65%
No surprise that additional therapy with an active drug led to improved PFS frankly, but 3 year PFS were 75% versus 65%

Before I tell you what IS interesting about this-
I want to tell you how for high-risk patients, on subset analysis benefits from almost every single intervention have been much attenuated. Even for len maintenance.
I want to tell you how for high-risk patients, on subset analysis benefits from almost every single intervention have been much attenuated. Even for len maintenance.
So their graph for high-risk here includes Gain 1q (which increases overall number of high-risk quite abit).
But in this graph- high-risk patients also had a PFS benefit with K-R maintenance, as previously presented at the IMW 2021 by @RobertoMinaMD
But in this graph- high-risk patients also had a PFS benefit with K-R maintenance, as previously presented at the IMW 2021 by @RobertoMinaMD
Admittedly, the supplement of this manuscript had a slightly underwhelming subset analysis of high-risk patients once the numbers are reduced (presumably Gain1q removed).
But still- seems to benefit overall.
But still- seems to benefit overall.

So what are we make of this?
Is K-R maintenance the new standard of care for everybody?
I would argue that there is still equipoise for len maintenance approaches outside and within clinical trials, as OS is gold standard.
Is K-R maintenance the new standard of care for everybody?
I would argue that there is still equipoise for len maintenance approaches outside and within clinical trials, as OS is gold standard.
Trials like DRAMMATIC looking at diff maint approaches/de-escalation and powered for OS are fantastic.
I am not so sure about this selinexor+len versus len maintenance with endpoint of PFS anymore though.
If youre powering for PFS, umm you know KR gives you better PFS.
I am not so sure about this selinexor+len versus len maintenance with endpoint of PFS anymore though.
If youre powering for PFS, umm you know KR gives you better PFS.

Will I do K+R maintenance for all- NO.
Does this add to the body of lower quality evidence preceding this that high-risk patients should have a PI as part of their maintenance-YES
Does it tell us KRD is better than VRD- NO
Should we put too much weight in a single MRD neg-NO
Does this add to the body of lower quality evidence preceding this that high-risk patients should have a PI as part of their maintenance-YES
Does it tell us KRD is better than VRD- NO
Should we put too much weight in a single MRD neg-NO
And finally- can we write off auto-transplant in the era of newer/sexier drugs like carfilzomib.
Ummm- NO.
Ummm- NO.
So, for those who braved through this long thread- kudos to you. Tons to process and learn, and I would love your feedback.
Thank you!
Thank you!
@RahulBanerjeeMD @amarkelkar @HiraSMian @AaronGoodman33 @ShoMidha @rajshekharucms @TMSchmidtMD @HadidiSamer @BldCancerDoc
Tagging some of the myeloma/transplant peeps for their thoughts and feedback!
Tagging some of the myeloma/transplant peeps for their thoughts and feedback!
• • •
Missing some Tweet in this thread? You can try to
force a refresh