COVID Update: At a time when most scientists are concluding an additional mRNA vaccines is needed, a Republican senator wants to go the other direction.
His idea? Prior infection should count as immunity. 1/
His idea? Prior infection should count as immunity. 1/
Roger Marshall from Kansas thinks the country should officially recognize prior COVID infection as the equivalent of being vaccinated when considering a vaccine requirement.
He’s not alone but he’s wrong in so many ways. 2/
He’s not alone but he’s wrong in so many ways. 2/
Roger also recently said this:
“The people that have thus far not gotten the vaccine are not going to do it until this White House acknowledges natural immunity.”
He’s calling for a sort of protest? Wut? 3/
“The people that have thus far not gotten the vaccine are not going to do it until this White House acknowledges natural immunity.”
He’s calling for a sort of protest? Wut? 3/
Several Republican states have in fact passed or are passing laws allowing prior infection with COVID to count the same as a vaccination as @JoanneKenen from @politico has pointed out. 4/
I will grant that Kansas Senator Roger Marshall is an OB/Gyn.
Another description of an OB/Gyn is “still not an infectious disease expert.” And it’s the confusion between illness & infection that leads Roger astray.
5/
Another description of an OB/Gyn is “still not an infectious disease expert.” And it’s the confusion between illness & infection that leads Roger astray.
5/
Let’s look at his claims. There are 10s of millions of unvaxxed Americans with prior infection. Prior infection provides them some protection in 2 ways.
-a shorter term & targeted antibody response
-a T cell response to protect against more serious illness 6/
-a shorter term & targeted antibody response
-a T cell response to protect against more serious illness 6/
Let’s look at those both with a little more rigor than Roger has.
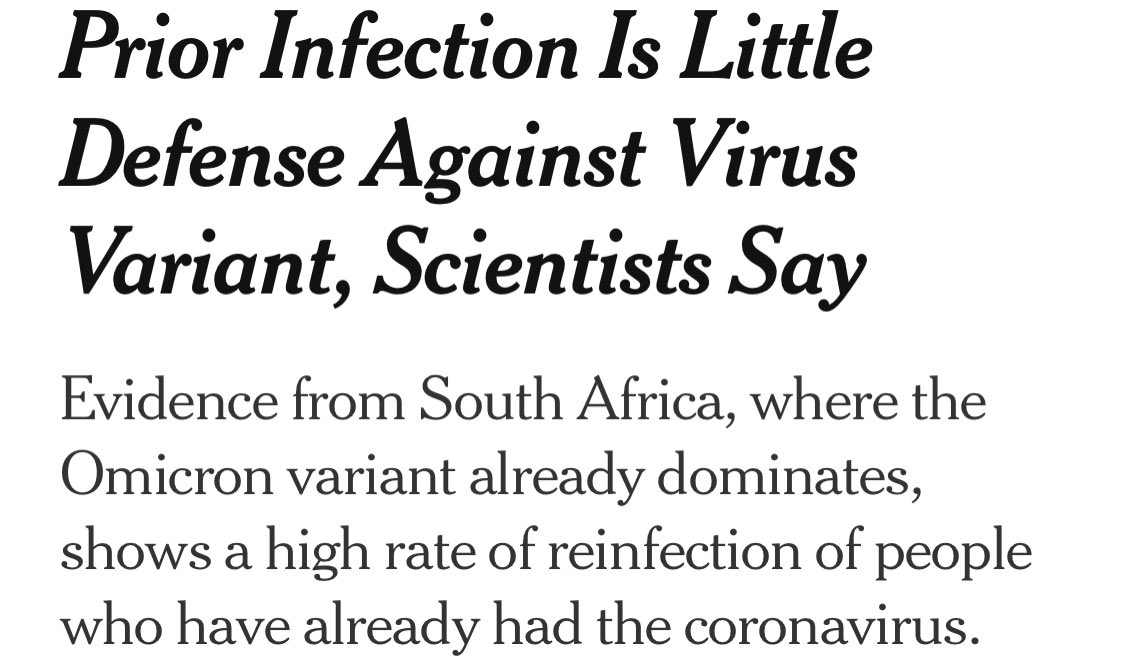
First, the short term targeted antibody response, while real, is, well, short term.
And it’s also targeted. Meaning Delta infection doesn’t create enough antibodies against Omicron. 7/
uclahealth.org/u-magazine/cor…
First, the short term targeted antibody response, while real, is, well, short term.
And it’s also targeted. Meaning Delta infection doesn’t create enough antibodies against Omicron. 7/
uclahealth.org/u-magazine/cor…

The second benefit is a T cell or memory B cell response that initiates later & aims to prevent an upper respiratory infection from traveling to the lungs.
While this is a great feature of the immune system, it is 100% irrelevant here. 8/
While this is a great feature of the immune system, it is 100% irrelevant here. 8/
Vaccine requirements aren’t concerned with unvaccinated people’s illness from spreading to their lungs. They are concerned with the virus spreading to OTHER PEOPLE.
Roger, that’s why people care— because it’s an INFECTIOUS disease. 9/
Roger, that’s why people care— because it’s an INFECTIOUS disease. 9/
This is an ongoing misconception among people who don’t support vaccine or mask requirements in any situation.
If someone were able to get COVID & not spread it, nobody would care whether you took care of yourself. It’s because you can make us sick. 10/
If someone were able to get COVID & not spread it, nobody would care whether you took care of yourself. It’s because you can make us sick. 10/
Your illness, your business.
You spreading your illness to the rest of us including kids, older people & sick people, that’s everyone’s business. 11/
You spreading your illness to the rest of us including kids, older people & sick people, that’s everyone’s business. 11/
And if you haven’t heard, COVID (Delta and Omicron both) are very contagious. According to @larrybrilliant, accounting for the quick incubation period, they make COVID the fastest spreading respiratory illness ever recorded. 12/
But, some say, it’s getting less lethal, more like the flu. Why make a big deal over spreading it?
First, what kind of person is OK spreading the flu?
Second, there’s no evidence that Omicron will be less lethal. And even if it turns out to be, it won’t be for everybody.13/
First, what kind of person is OK spreading the flu?
Second, there’s no evidence that Omicron will be less lethal. And even if it turns out to be, it won’t be for everybody.13/
So prior infection may for help the individual but it doesn’t do much to help the rest of us.
And I haven’t heard how Roger thinks we will verify whether someone has had a prior infection. Because he really doesn’t think we should. He’s just mucking up the gears. 14/
And I haven’t heard how Roger thinks we will verify whether someone has had a prior infection. Because he really doesn’t think we should. He’s just mucking up the gears. 14/
So what is Roger really saying? He’s saying to unvaccinated people that they should be able tell everyone else to just fuck off.
And part of that brave stance is to be OK getting COVID. And not afraid to give the infection to someone else. 15/
And part of that brave stance is to be OK getting COVID. And not afraid to give the infection to someone else. 15/
A more responsible person would let the health authorities parse this complex topic for people.
But Roger’s aim isn’t better public health understanding. His comments were made prior to his vote to strip OSHA of its authorities to require workplaces protect against COVID. 16/
But Roger’s aim isn’t better public health understanding. His comments were made prior to his vote to strip OSHA of its authorities to require workplaces protect against COVID. 16/
Aren’t vaccines subject to similar properties? Waning and some level of reinfection?
Less so but yes— particularly against Omicron. So we will need to consider what the science is likely to tell us about Omicron. 17/
Less so but yes— particularly against Omicron. So we will need to consider what the science is likely to tell us about Omicron. 17/
Particularly once Omicron hits US shores in earnest, the CDC & local public health authorities must revisit their definition of vaccinated— likely to require an mRNA booster.
And if the science later tells us we will need a different shot, we need to look at that too. 18/
And if the science later tells us we will need a different shot, we need to look at that too. 18/
Many will come out and say— see if the science changes, don’t trust it.
Others will say that the science evolving as the virus changes is why we trust it. 19/
Others will say that the science evolving as the virus changes is why we trust it. 19/
Around the globe this could also mean that shots of Sinopharm or Sputnik or AZ, could also be insufficient.
This will mean higher cases & losses around the world. It could also mean proof of vax requirements to travel will need to evolve. 20/
This will mean higher cases & losses around the world. It could also mean proof of vax requirements to travel will need to evolve. 20/
We have the tools today to minimize the virus’s impact if we use them.
At this point in the pandemic we should be preparing to take on tomorrow’s challenges not fighting anti-science propaganda. /end
At this point in the pandemic we should be preparing to take on tomorrow’s challenges not fighting anti-science propaganda. /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh